Tuesday, 25 December 2012
Have a very healthy Christmas!
Happy Christmas everyone! Thanks for reading my blog over the past year. No doubt there'll be much more to tell in the new year. I hope your holidays are both happy and healthy! xxx
Monday, 24 December 2012
How Not To Get A Date
So there's quite a lot of catching-up to do, given that I have been a bad pituitary blogger for the past month and a half and yet quite a few highly relevant things have happened, including meeting with the neurosurgeon and Ear Nose and Throat people (who are apparently more properly called Otolaryngologists - who knew?) and finally getting a date for surgery. I shall start at the very beginning...
At the beginning of November, my next injection was due. You probably know by now that I need monthly injections of lanreotide, a somatostatin analogue, to suppress the overproduction of thyroid stimulating hormone by my pituitary tumour. These injections are delivered into my hip via the medium of a really big needle. It's so big I'm pretty sure a camel actually could pass through it.*
One of the nurses greeted me when I arrived, took my bloods and then went to get the injection. Then something happened which had never happened before.
"Would you like any freezing spray?" she asked me.
I was nonplussed. Previously, I had always associated freezing spray with childhood trips to the Irish seaside, not hospitals. I had to ask what it was.
"Oh, it's just a spray which freezes the skin before an injection," the nurse explained.
Those who know me well will know that one of the few things I like less than injections is being cold. "Sounds unpleasant," I said.
"Yes, it's quite painful," the nurse said breezily. "But some patients still prefer it."
Now at this point, I admit perhaps I should have smelled a rat. No other nurse had ever offered me freezing spray prior to one of these injections. But I wasn't worried.
Like a fool.
Most nurses, when they do this injection, hold the needle (did I mention it's massive?) against your skin and then gently press it in. Not this nurse. Instead, she opted to hold the needle some distance away from the injection site, then take a great swing and stab me with it. It was considerably more painful than usual, and I bled a lot more than normal as well.
I can see why her patients usually ask for freeze spray.
So, I promptly became the proud owner of an excitingly multi-coloured hip bruise, which lasted for three weeks before finally fading just before I was due the next injection. I actually did try to take a photo to show you all but it just came out as a blurry smoosh. For a couple of days I couldn't even lie in bed on that side without wincing.
Anyway, that anecdote was by way of being an aperitif to the main cock-up that I encountered on that trip to the hospital. While my hip was bleeding gently, one of the endocrine nurses asked if I'd heard
anything from the Neurosurgery or Ear Nose & Throat departments, who were supposed to be getting in touch with me about my impending surgery. I explained that I'd still heard nothing and that despite my attempts to call them I'd never got through to speak to an actual human being, and they'd never returned any of my messages. The nurse went off, had a look at her computer, and returned to tell me that I'd had an appointment with ENT. On the 26th October. Which was four days previously.
I also had an appointment booked in on the 5th November with Neurosurgery which I knew nothing about, and ENT had written to me to rearrange my missed appointment for the 6th November.
They'd been writing to my old address.
I still don't have the faintest idea how it happened. As soon as I moved house, I duly phoned the hospital and updated them with my new address. Not long afterwards, I received an appointment from the MRI Department at my new house. I sighed a deep sigh of relief in the happy knowledge
that my details had been successfully updated... and it never occurred to me that they might be sending appointments to my old address.
Obviously I am also slightly put out at my former housemates, who knew I was going to have surgery and who I'd asked to forward on any hospital-looking letters, or even just let me know if they arrived so that I could drop by to pick them up. But how the hospital could get it right... and then revert to getting it wrong, I have no idea. It's not the first time it's happened, either - avid readers will recall that information about a ream of tests I had to have in July was sent to my old address despite the fact that I'd not lived there in four months and all my other letters had gone through correctly.
So obviously, I was very upset about this. I had been doing everything I could to find out
about my appointments, and no-one ever got back to me. You have to wonder how many appointments I would have had to miss before anyone bothered to do so.
__________________________________
* Hell yeah, I'm cultured.
At the beginning of November, my next injection was due. You probably know by now that I need monthly injections of lanreotide, a somatostatin analogue, to suppress the overproduction of thyroid stimulating hormone by my pituitary tumour. These injections are delivered into my hip via the medium of a really big needle. It's so big I'm pretty sure a camel actually could pass through it.*
One of the nurses greeted me when I arrived, took my bloods and then went to get the injection. Then something happened which had never happened before.
"Would you like any freezing spray?" she asked me.
I was nonplussed. Previously, I had always associated freezing spray with childhood trips to the Irish seaside, not hospitals. I had to ask what it was.
"Oh, it's just a spray which freezes the skin before an injection," the nurse explained.
Those who know me well will know that one of the few things I like less than injections is being cold. "Sounds unpleasant," I said.
"Yes, it's quite painful," the nurse said breezily. "But some patients still prefer it."
Now at this point, I admit perhaps I should have smelled a rat. No other nurse had ever offered me freezing spray prior to one of these injections. But I wasn't worried.
Like a fool.
Most nurses, when they do this injection, hold the needle (did I mention it's massive?) against your skin and then gently press it in. Not this nurse. Instead, she opted to hold the needle some distance away from the injection site, then take a great swing and stab me with it. It was considerably more painful than usual, and I bled a lot more than normal as well.
I can see why her patients usually ask for freeze spray.
So, I promptly became the proud owner of an excitingly multi-coloured hip bruise, which lasted for three weeks before finally fading just before I was due the next injection. I actually did try to take a photo to show you all but it just came out as a blurry smoosh. For a couple of days I couldn't even lie in bed on that side without wincing.
Anyway, that anecdote was by way of being an aperitif to the main cock-up that I encountered on that trip to the hospital. While my hip was bleeding gently, one of the endocrine nurses asked if I'd heard
anything from the Neurosurgery or Ear Nose & Throat departments, who were supposed to be getting in touch with me about my impending surgery. I explained that I'd still heard nothing and that despite my attempts to call them I'd never got through to speak to an actual human being, and they'd never returned any of my messages. The nurse went off, had a look at her computer, and returned to tell me that I'd had an appointment with ENT. On the 26th October. Which was four days previously.
I also had an appointment booked in on the 5th November with Neurosurgery which I knew nothing about, and ENT had written to me to rearrange my missed appointment for the 6th November.
They'd been writing to my old address.
I still don't have the faintest idea how it happened. As soon as I moved house, I duly phoned the hospital and updated them with my new address. Not long afterwards, I received an appointment from the MRI Department at my new house. I sighed a deep sigh of relief in the happy knowledge
that my details had been successfully updated... and it never occurred to me that they might be sending appointments to my old address.
Obviously I am also slightly put out at my former housemates, who knew I was going to have surgery and who I'd asked to forward on any hospital-looking letters, or even just let me know if they arrived so that I could drop by to pick them up. But how the hospital could get it right... and then revert to getting it wrong, I have no idea. It's not the first time it's happened, either - avid readers will recall that information about a ream of tests I had to have in July was sent to my old address despite the fact that I'd not lived there in four months and all my other letters had gone through correctly.
So obviously, I was very upset about this. I had been doing everything I could to find out
about my appointments, and no-one ever got back to me. You have to wonder how many appointments I would have had to miss before anyone bothered to do so.
__________________________________
* Hell yeah, I'm cultured.
Sunday, 23 December 2012
Sprouts: A Festive Warning
Regular readers - and anyone who's ever had a roast dinner with me - will be aware of my aversion to Brussels sprouts. I might go so far as to call it a hatred of them.
And finally I have conclusive proof that eating sprouts is bad to for you (albeit only under highly specific conditions): a man was hospitalised last Christmas after eating too many Brussels sprouts. Sprouts contain a very high level of vitamin K, which promotes blood clotting and as a result of the sheer amount of sprouts the poor man had eaten, the high levels of vitamin K served to counteract the effect of the anticoagulants he was taking due to heart failure.
Docftors were baffled as to why the medication wasn't working until, presumably, one of them smelled him.
And finally I have conclusive proof that eating sprouts is bad to for you (albeit only under highly specific conditions): a man was hospitalised last Christmas after eating too many Brussels sprouts. Sprouts contain a very high level of vitamin K, which promotes blood clotting and as a result of the sheer amount of sprouts the poor man had eaten, the high levels of vitamin K served to counteract the effect of the anticoagulants he was taking due to heart failure.
Docftors were baffled as to why the medication wasn't working until, presumably, one of them smelled him.
 |
| DANGER! DANGER! |
Saturday, 22 December 2012
Pituitary Awareness Quiz: The Results
I was so impressed by how many of you took part in my little quiz - apologies for the long delay in coming out and praising you for it! Some people dipped in and out for the odd question, while others were with us for the long haul.
Bearing in mind that double points were awarded for witty answers rather than merely correct ones, I present... The Results!
The winner is... Clare! With the close runner-up Davey D. Congratulations guys, you may officially brag wildly about your knowledge of the pituitary gland and its inhabitants.
And as I did promise a praise poem for the winner:
There was a young lady named Clare
As wise (and fierce) as an owlbear.
She was a quiz queen
- quite the answer machine -
she made other contestants despair!
Bearing in mind that double points were awarded for witty answers rather than merely correct ones, I present... The Results!
THE RESULTS
The winner is... Clare! With the close runner-up Davey D. Congratulations guys, you may officially brag wildly about your knowledge of the pituitary gland and its inhabitants.
And as I did promise a praise poem for the winner:
There was a young lady named Clare
As wise (and fierce) as an owlbear.
She was a quiz queen
- quite the answer machine -
she made other contestants despair!
Friday, 21 December 2012
Pituitary Awareness Quiz: The Answers
Hola! Well, I'm just back from a spot of festive carol singing at the local pub with my whole family in tow, and I thought: what better time to finally put up the answers to October's National Pituitary Month quiz?
Q.1: Acromegaly is a rare disease caused by a growth-hormone-secreting pituitary tumour, which can lead to gigantism and excessive growth of the body's tissues. But what language is the word "acromegaly" derived from, and what does it literally mean?
Correct answer: c) from the Greek akros "highest; extremity" and megalos "large".
***
Q.2: Approximately how many (normal-sized) human pituitary glands could you fit in an Olympic-sized swimming pool?
Correct answer: Wildly debateable! Although I did have a correct answer, calculated by my lovely boyfriend on the basis of the human pituitary gland being roughly the size of a pea and assuming that the glands on the bottom retained their shape instead of being pulverized by the weight of the ones on top, I decided to award a point to anyone who showed their working; because it's the effort that counts!
***
Q.3: Which of these is an alternative name for the pituitary stalk?
Correct answer: c) The infundibular stem
***
Q.4: The human pituitary gland will vary in size over a person's life. What physiological event (other than untoward tumourousness) causes the pituitary gland to reach its largest natural size... and why?
Correct answer: Pregnancy, although the gland tends to be at its largest shortly after giving birth. This is due to lactotroph hyperplasia; basically that means an increase in the number of cells which secrete the hormone prolactin, which stimulates milk production for breastfeeding.
***
Q.5: Beta-endorphin is used by the body to numb pain, and is found in the anterior pituitary gland, as well as the hypothalamus. From the extracts of which species' pituitary gland was beta-endorphin first discovered?
Correct answer: d) Camel (apparently!)
***
***
Q.8: I'm currently receiving monthly lanreotide injections. These are somatostatin analogues - hormone injections - which counteract the effect of my pituitary adenoma producing too much thyroid hormone. Assuming this is the only medication I'm taking, and assuming I live in England... am I allowed to donate blood?
Correct answer: a) Yes
***
Q.9: Which of the below is the correct spelling of the full name of the pituitary hormone ACTH? (no cheating!)
Correct answer: d) adrenocorticotropic hormone
***
Q.10: What hormone does my pituitary tumour overproduce?
Correct answer: a) Thyroid stimulating hormone
***
Q.11: Who is this man, and what does he have to do with the pituitary gland?
Correct answer: Harvey Cushing, pioneering neurosurgeon and the man who discovered Cushing's Syndrome.
***
So now you know!
The results will be out tomorrow...
THE ANSWERS:
Q.1: Acromegaly is a rare disease caused by a growth-hormone-secreting pituitary tumour, which can lead to gigantism and excessive growth of the body's tissues. But what language is the word "acromegaly" derived from, and what does it literally mean?
Correct answer: c) from the Greek akros "highest; extremity" and megalos "large".
***
Q.2: Approximately how many (normal-sized) human pituitary glands could you fit in an Olympic-sized swimming pool?
Correct answer: Wildly debateable! Although I did have a correct answer, calculated by my lovely boyfriend on the basis of the human pituitary gland being roughly the size of a pea and assuming that the glands on the bottom retained their shape instead of being pulverized by the weight of the ones on top, I decided to award a point to anyone who showed their working; because it's the effort that counts!
***
Q.3: Which of these is an alternative name for the pituitary stalk?
Correct answer: c) The infundibular stem
***
Q.4: The human pituitary gland will vary in size over a person's life. What physiological event (other than untoward tumourousness) causes the pituitary gland to reach its largest natural size... and why?
Correct answer: Pregnancy, although the gland tends to be at its largest shortly after giving birth. This is due to lactotroph hyperplasia; basically that means an increase in the number of cells which secrete the hormone prolactin, which stimulates milk production for breastfeeding.
***
Q.5: Beta-endorphin is used by the body to numb pain, and is found in the anterior pituitary gland, as well as the hypothalamus. From the extracts of which species' pituitary gland was beta-endorphin first discovered?
Correct answer: d) Camel (apparently!)
***
Q.6: Only one of the following pituitary-related
conditions was first identified by a woman named Cindy. But which one was
it?
Correct answer: a) Sheehan Syndrome
***
Q.7: A five point bonus was awarded for writing a poem about the pituitary: there are no wrong answers!
Correct answer: a) Sheehan Syndrome
***
Q.7: A five point bonus was awarded for writing a poem about the pituitary: there are no wrong answers!
***
Q.8: I'm currently receiving monthly lanreotide injections. These are somatostatin analogues - hormone injections - which counteract the effect of my pituitary adenoma producing too much thyroid hormone. Assuming this is the only medication I'm taking, and assuming I live in England... am I allowed to donate blood?
Correct answer: a) Yes
***
Q.9: Which of the below is the correct spelling of the full name of the pituitary hormone ACTH? (no cheating!)
Correct answer: d) adrenocorticotropic hormone
***
Q.10: What hormone does my pituitary tumour overproduce?
Correct answer: a) Thyroid stimulating hormone
***
Q.11: Who is this man, and what does he have to do with the pituitary gland?
Correct answer: Harvey Cushing, pioneering neurosurgeon and the man who discovered Cushing's Syndrome.
***
So now you know!
The results will be out tomorrow...
Wednesday, 12 December 2012
Back to the Blog!
It has been a horrendously long time since I wrote on here! So much has
happened in the intervening month-and-a-bit, so I apologise. I'm afraid
my November-based absence is down to a vague attempt to complete
National Novel Writing Month, combined with a set of professional exams
at the end of November. As it happens, I failed to complete my 50,000
word novel and I think probably managed to fail an exam as well, so my
abandonment was entirely pointless; I might as well have just kept
blogging! Additionally I am not assisted by changed to blogger which
mean that it no longer works at all with faintly elderly versions of
Internet Explorer, which means that I can no longer post updates during
my lunch hour at work.
Anyway, many and greater updates must wait for another day, alas - however, I can share the exciting news that I am currently scheduled to have another bout of transsphenoidal pituitary surgery on the 15th January.
Yes, that is only just over a month away! But more on that some other time...
Anyway, many and greater updates must wait for another day, alas - however, I can share the exciting news that I am currently scheduled to have another bout of transsphenoidal pituitary surgery on the 15th January.
Yes, that is only just over a month away! But more on that some other time...
Wednesday, 31 October 2012
Pituitary Awareness Quiz: The final day!
Thanks to everyone who has partaken of the quiz! Today is not just Halloween, it's also the end of National Pituitary Awareness Month, which is obviously both far more important and far more tragic. Hopefully you have been educated and enthralled; probably not, but I am deeply optimistic. Today is your last chance to answer any questions you haven't answered yet - then tomorrow I shall publish the correct answers and, of course, the winner!
And as a Halloween bonus, you cannot fail to gain a point today :)
Q.11: Have you learned anything about the pituitary gland from taking part in this quiz?
a) Yes
b) Indeed
And as a Halloween bonus, you cannot fail to gain a point today :)
Pituitary Awareness Quiz
Day 11, Question 11
Q.11: Have you learned anything about the pituitary gland from taking part in this quiz?
a) Yes
b) Indeed
Tuesday, 30 October 2012
Pituitary Awareness Quiz: Day 11
Pituitary Awareness Quiz
Day 11, Question 11
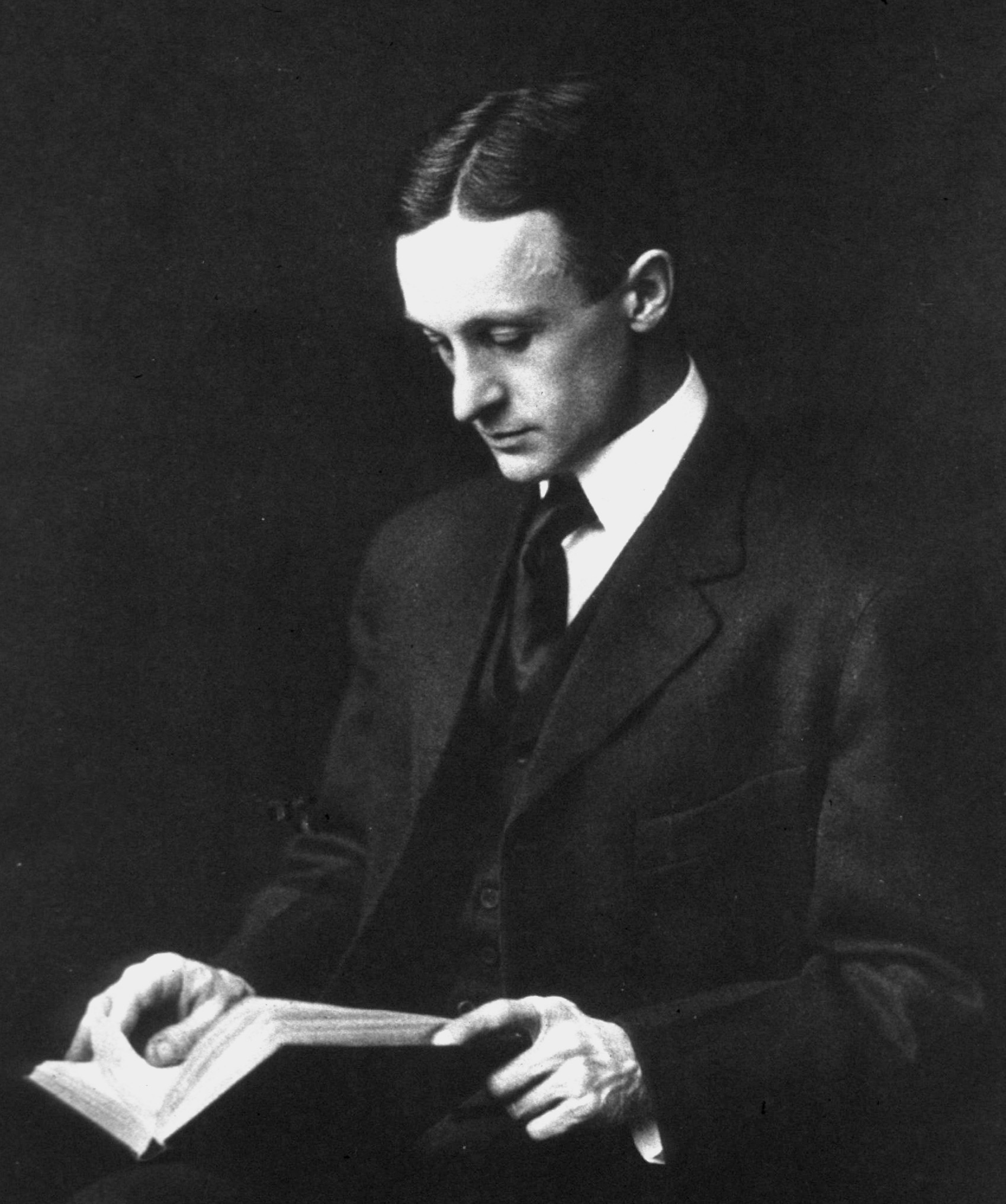
Q.11: Who is this man, and what does he have to do with the pituitary gland? No multiple-choice today I'm afraid... you're on your own!
Monday, 29 October 2012
Pituitary Awareness Quiz: Day 10
Another day missed! Apologies. I do have an exciting update but I'm not sure I'm up to typing it all this evening. Consequently, I present today's super simple question:
Q.10: What hormone does my pituitary tumour overproduce?
a) Thyroid stimulating hormone
b) Thyrotropin releasing hormone
c) Thyroid hormone
Pituitary Awareness Quiz
Day 10, Question 10
Q.10: What hormone does my pituitary tumour overproduce?
a) Thyroid stimulating hormone
b) Thyrotropin releasing hormone
c) Thyroid hormone
Saturday, 27 October 2012
Pituitary Awareness Quiz: Day 9
Eagle-eyed readers will have noted that this is in fact Day 10, but I abjectly failed to write a question yesterday (though I did write a poem, which is nearly as good) so it's only question nine. I could have called this Day 10, Question 9, but that just seems confusing so I'm working on the basis that yesterday was just a small aberration in time and space, and the quiz will continue from here!
Q.9: Which of the below is the correct spelling of the full name of the pituitary hormone ACTH? (no cheating!)
a) adrenalcortecotropic hormone
b) adrenecorticotropic hormone
c) adrenalcorticotropic hormone
d) adrenocorticotropic hormone
Pituitary Awareness Quiz
Day 9, Question 9
Q.9: Which of the below is the correct spelling of the full name of the pituitary hormone ACTH? (no cheating!)
a) adrenalcortecotropic hormone
b) adrenecorticotropic hormone
c) adrenalcorticotropic hormone
d) adrenocorticotropic hormone
Friday, 26 October 2012
Schrödinger's MRI Scan (A Hallowe'en Special)
Some time ago, I received an appointment from the hospital for an MRI scan on the 31st October. I immediately - and diligently - phoned them up to ask whether or not this was a mistake. I had been due to have a scan after three continuous months on my current medication, and due to delays in getting funding for my lanreotide injections, I'd not had one for two months at that point. I was told not to cancel the appointment, and that I would be informed of whether or not to go.
I've reminded them about this twice since, and both times been informed that I almost certainly won't need to have the scan on the 31st - because it would be wildly pointless - but that I shouldn't cancel it, and it will be rearranged.
Well, the scan is next Wednesday (on Hallowe'en, no less!) and I've still heard bugger all. I don't know what the cost of an MRI scan is to the NHS, but I do know that the scanners at my local hospital can sometimes be booked up months in advance, and for me to be hanging on to an appointment I don't need, or to have a scan that won't be particularly useful to my doctors, is stupid.
I was going to attempt to call and remind them about this at lunchtime today, but I was hit by a sudden feeling of futility and hopelessness, so I composed a poem about it instead.
***
My MRI on Wednesday is sure to be a blast
I'll have more scans in future; I've had some in the past.
But this one will be special, for there's something I don't know -
Nobody has informed me whether or not I should go!
I can't say if they're expecting me to turn up on the day,
Or whether they'll be angry if instead I stay away.
I'm caught in a Catch-22, for I've no way of knowing
if I should go (or not) until I am already going.
It's Schrödinger's MRI scan, with my head inside the box
I'm quantumly entangled like a cat (or like a fox.
The fox is very prone to being used in paradoxes
For it's fairly cute and docile, and it wears such tiny sockses.)
My scan is not alive, yet its brain function has not ended
In terms of animation, it is currently suspended.
Like Dracula, there's still a chance it may rise from the grave;
EEG scans indicate disrupted delta waves.
Perhaps, for Hallowe'en, the MRI team has decided
that they're sick of being left out, and cruelly derided
(The other hospital staff tend to laugh and call them names
because, you see, they claim all MRI scans look the same).
And consequently they've now all come up with this little caper
(Which I find about as funny as a piece of plain white paper)
They won't click "confirm appointment", neither will they click "delete"
And when I show up for my scan, they'll all shout: "Trick or treat!"
I've reminded them about this twice since, and both times been informed that I almost certainly won't need to have the scan on the 31st - because it would be wildly pointless - but that I shouldn't cancel it, and it will be rearranged.
Well, the scan is next Wednesday (on Hallowe'en, no less!) and I've still heard bugger all. I don't know what the cost of an MRI scan is to the NHS, but I do know that the scanners at my local hospital can sometimes be booked up months in advance, and for me to be hanging on to an appointment I don't need, or to have a scan that won't be particularly useful to my doctors, is stupid.
I was going to attempt to call and remind them about this at lunchtime today, but I was hit by a sudden feeling of futility and hopelessness, so I composed a poem about it instead.
***
My MRI on Wednesday is sure to be a blast
I'll have more scans in future; I've had some in the past.
But this one will be special, for there's something I don't know -
Nobody has informed me whether or not I should go!
I can't say if they're expecting me to turn up on the day,
Or whether they'll be angry if instead I stay away.
I'm caught in a Catch-22, for I've no way of knowing
if I should go (or not) until I am already going.
It's Schrödinger's MRI scan, with my head inside the box
I'm quantumly entangled like a cat (or like a fox.
The fox is very prone to being used in paradoxes
For it's fairly cute and docile, and it wears such tiny sockses.)
My scan is not alive, yet its brain function has not ended
In terms of animation, it is currently suspended.
Like Dracula, there's still a chance it may rise from the grave;
EEG scans indicate disrupted delta waves.
Perhaps, for Hallowe'en, the MRI team has decided
that they're sick of being left out, and cruelly derided
(The other hospital staff tend to laugh and call them names
because, you see, they claim all MRI scans look the same).
And consequently they've now all come up with this little caper
(Which I find about as funny as a piece of plain white paper)
They won't click "confirm appointment", neither will they click "delete"
And when I show up for my scan, they'll all shout: "Trick or treat!"
Thursday, 25 October 2012
Pituitary Awareness Quiz: Day 8
I received one incredibly excellent poem in response to yesterday's question, I thoroughly encourage you all to go check it out! (And remember; it's never too late to respond!)
Today's question will be rather more staid and run-of-the-mill, however it may require a little detective work to find the right answer. Equally though, you have a fifty-fifty chance of getting it right without doing the legwork! But if you get it wrong, you'll look kind of foolish right? Hmm... tricksy.
Q.8: I'm currently receiving monthly lanreotide injections. These are somatostatin analogues - hormone injections - which counteract the effect of my pituitary adenoma producing too much thyroid hormone.
Assuming this is the only medication I'm taking, and assuming I live in England... am I allowed to donate blood?
a) Yes
b) No
Today's question will be rather more staid and run-of-the-mill, however it may require a little detective work to find the right answer. Equally though, you have a fifty-fifty chance of getting it right without doing the legwork! But if you get it wrong, you'll look kind of foolish right? Hmm... tricksy.
Pituitary Awareness Quiz
Day 8, Question 8
Q.8: I'm currently receiving monthly lanreotide injections. These are somatostatin analogues - hormone injections - which counteract the effect of my pituitary adenoma producing too much thyroid hormone.
Assuming this is the only medication I'm taking, and assuming I live in England... am I allowed to donate blood?
a) Yes
b) No
Wednesday, 24 October 2012
Pituitary Awareness Quiz: Day 7
Regular readers will be unsurprised to hear that I still have not heard back from the hospital about, you know, getting my surgery arranged or whether I need to go to the MRI I'm due to have in a week. I had a really special time on Friday when I tried to contact the neurosurgery clinic to find out what the heck was going on. It went something like this:
Attempt 1:
Hospital Employee 1: Hello, switchboard at The Hospital, how may I help?
Me: Hi, could you put me through to the neurosurgery clinic please?
Hospital Employee 1: (suddenly speaking s-l-o-w-l-y and clearly) Yes, of course, I'll put you through now.
(A pause. The phone rings.)
Hospital Employee 2: Hello, Dermatology department. How can I help?
Attempt 2:
Hospital Employee 1: Hello, switchboard at The Hospital, how may I help?
Me: Hi, I just called to be put through to neurosurgery but I ended up on the dermatology phone instead?
Hospital Employee 1: Oh, sorry about that. I'll just connect you now.
(A pause. The phone rings.)
(For like five minutes, then I gave up)
On attempt 3 I got through to the Neuroscience answering machine and left a message, but I'm not hugely sanguine about the results, especially as they've now had three days to phone me. Oi vey!
Anyway, today's question is a more creative question. Presenting:
Attempt 1:
Hospital Employee 1: Hello, switchboard at The Hospital, how may I help?
Me: Hi, could you put me through to the neurosurgery clinic please?
Hospital Employee 1: (suddenly speaking s-l-o-w-l-y and clearly) Yes, of course, I'll put you through now.
(A pause. The phone rings.)
Hospital Employee 2: Hello, Dermatology department. How can I help?
Attempt 2:
Hospital Employee 1: Hello, switchboard at The Hospital, how may I help?
Me: Hi, I just called to be put through to neurosurgery but I ended up on the dermatology phone instead?
Hospital Employee 1: Oh, sorry about that. I'll just connect you now.
(A pause. The phone rings.)
(For like five minutes, then I gave up)
On attempt 3 I got through to the Neuroscience answering machine and left a message, but I'm not hugely sanguine about the results, especially as they've now had three days to phone me. Oi vey!
Anyway, today's question is a more creative question. Presenting:
Pituitary Awareness Quiz
Day 7, Question 7
Q.7: I will be awarding a SPECTACULAR bonus of no less than FIVE POINTS to anyone who can write me a short poem (two lines is sufficient) about/vaguely related to the pituitary. Bonus points for anyone who finds a rhyme for "pituitary"!
Tuesday, 23 October 2012
Pituitary Awareness Quiz: Day 6
Yesterday's animal-based question proved wildly unpopular. So I thought I'd leave animal-based questions behind and go for a classic history lesson set-up!
National Pituitary Awareness Month Pituitary Awareness Quiz
Day 6, Question 6
Q.6: Only one of the following pituitary-related conditions was first identified by a woman named Cindy. But which one was it?
a) Sheehan Syndrome
b) Cushing's Syndrome
c) Addison's Disease
d) Pituitary apoplexy
a) Sheehan Syndrome
b) Cushing's Syndrome
c) Addison's Disease
d) Pituitary apoplexy
Monday, 22 October 2012
Pituitary Awareness Quiz: Day 5
Aloha! Today's question is rather late, I very nearly forgot to write it at all. Nearly... but not quite! The nice thing about doing this quiz has been that I've also learned things about the pituitary and its various hormones that I never knew before. And so, ladies and gentlemen, I present:
Q.5: Beta-endorphin is used by the body to numb pain, and is found in the anterior pituitary gland, as well as the hypothalamus. From the extracts of which species' pituitary gland was beta-endorphin first discovered?
a) Dolphin
b) Guinea Pig
c) Chimp
d) Camel
e) Owlbear
National Pituitary Awareness Month Pituitary Awareness Quiz
Day 5, Question 5
Q.5: Beta-endorphin is used by the body to numb pain, and is found in the anterior pituitary gland, as well as the hypothalamus. From the extracts of which species' pituitary gland was beta-endorphin first discovered?
a) Dolphin
b) Guinea Pig
c) Chimp
d) Camel
e) Owlbear
 |
| Bonus Question: How do you extract an owlbear's pituitary? |
Sunday, 21 October 2012
Growth Hormone and Creutzfeldt-Jakob Disease
It's National Pituitary Awareness Month, and I thought I should look for an interesting pituitary-related story to tell you all. As it turned out, I didn't have to look too far.
Most people living in Britain today will remember the 1996 scare about "mad cow disease" or BSE (in cows the disease is called Bovine Spongiform Encephalopathy; when it's passed to humans it's variant Creutzfeldt-Jakob Disease or vCJD). It’s an extremely nasty degenerative brain disease, invariably fatal, and there was huge concern that beef contaminated with the disease had been in the food chain for some time. The illness can have a latency period of up to ten years before symptoms appear (or much, much longer according to some researchers), making it very difficult to trace the cause of the illness - and meaning that no-one has any definite idea how many people could have been infected. As of October 2009, there had been 166 identified cases of the illness in the UK.
It was a huge scandal in the UK, and I remember as a child being disappointed that I wasn't allowed to eat roast beef for what felt like a very long time - although admittedly this was less because I loved roast beef and more because I loved the accompanying Yorkshire pudding my mum served with it. But until recently I was not aware of a similar, albeit smaller-scale scandal that had occurred several years earlier.
Between 1963 and 1985, the US Government funded a programme which provided human growth hormone to children across the US who had failed to grow as expected. Failure to grow in children is sometimes due to a deficiency in growth hormone (surprise!) and this is still a treatment for children today; the difference is that these days it's made in a lab, while at that time it was extracted directly from the pituitary glands of human cadavers.
In 1985, it came to light that three of the people treated with human growth hormone (hGH) had gone on to die of Creutzfeldt-Jakob Disease. This is not the same illness as vCJD but it is similar - and it's very, very rare. The programme was stopped immediately and an investigation launched.
To date, 29 of the people treated with hGH in the US before 1977 have been diagnosed with CJD. That's about one in 95. The rates were much higher in some other countries; in the UK, which produced its own hGH, 64 of the 1849 people treated developed CJD; and in France, which also produced its own hGH, 119 out of 1700 patients went on to develop the disease. There have been cases reported in numerous other countries; the variation in incidence is likely due to the variation in the way the hormone was extracted and processed.
The longest latency period recorded between someone receiving human Growth Hormone and going on to develop CJD is 38 years. The shortest period before developing symptoms with these kind of diseases is usually around 2 - 3 years. The symptoms progress very quickly, within just a few months, from dizziness, difficulty balancing and clumsiness to memory loss, seizures and death.
Most disturbingly of all, however, it later came to light that far more of the patients who had been treated with hGH went on to die of adrenal crisis - an entirely treatable problem - than of CJD. This problem isn't caused by the hGH treatment, it's simply the case that people with a growth hormone deficiency are more likely to also be deficient in other pituitary hormones, such as ACTH. Without sufficient ACTH, you will die - but safe and effective hormone replacement is available for people whose bodies don't produce enough ACTH. It's simply that their doctors failed to pick up on the fact that these people were ACTH-deficient until it was too late.
Most people living in Britain today will remember the 1996 scare about "mad cow disease" or BSE (in cows the disease is called Bovine Spongiform Encephalopathy; when it's passed to humans it's variant Creutzfeldt-Jakob Disease or vCJD). It’s an extremely nasty degenerative brain disease, invariably fatal, and there was huge concern that beef contaminated with the disease had been in the food chain for some time. The illness can have a latency period of up to ten years before symptoms appear (or much, much longer according to some researchers), making it very difficult to trace the cause of the illness - and meaning that no-one has any definite idea how many people could have been infected. As of October 2009, there had been 166 identified cases of the illness in the UK.
 |
| Beware! This could be a mad cow. |
Between 1963 and 1985, the US Government funded a programme which provided human growth hormone to children across the US who had failed to grow as expected. Failure to grow in children is sometimes due to a deficiency in growth hormone (surprise!) and this is still a treatment for children today; the difference is that these days it's made in a lab, while at that time it was extracted directly from the pituitary glands of human cadavers.
In 1985, it came to light that three of the people treated with human growth hormone (hGH) had gone on to die of Creutzfeldt-Jakob Disease. This is not the same illness as vCJD but it is similar - and it's very, very rare. The programme was stopped immediately and an investigation launched.
To date, 29 of the people treated with hGH in the US before 1977 have been diagnosed with CJD. That's about one in 95. The rates were much higher in some other countries; in the UK, which produced its own hGH, 64 of the 1849 people treated developed CJD; and in France, which also produced its own hGH, 119 out of 1700 patients went on to develop the disease. There have been cases reported in numerous other countries; the variation in incidence is likely due to the variation in the way the hormone was extracted and processed.
The longest latency period recorded between someone receiving human Growth Hormone and going on to develop CJD is 38 years. The shortest period before developing symptoms with these kind of diseases is usually around 2 - 3 years. The symptoms progress very quickly, within just a few months, from dizziness, difficulty balancing and clumsiness to memory loss, seizures and death.
Most disturbingly of all, however, it later came to light that far more of the patients who had been treated with hGH went on to die of adrenal crisis - an entirely treatable problem - than of CJD. This problem isn't caused by the hGH treatment, it's simply the case that people with a growth hormone deficiency are more likely to also be deficient in other pituitary hormones, such as ACTH. Without sufficient ACTH, you will die - but safe and effective hormone replacement is available for people whose bodies don't produce enough ACTH. It's simply that their doctors failed to pick up on the fact that these people were ACTH-deficient until it was too late.
Pituitary Awareness Quiz: Day 4
And we're on to day four! Today I have chosen not to do a multiple choice question, which is perhaps slightly evil - but equally it's a fairly easy question, so you should be fine. Ready, set.... Google!
Q.4: The human pituitary gland will vary in size over a person's life. What physiological event (other than untoward tumourousness) causes the pituitary gland to reach its largest natural size... and why?
National Pituitary Awareness Month Pituitary Awareness Quiz
Day 4, Question 4
Day 4, Question 4
Q.4: The human pituitary gland will vary in size over a person's life. What physiological event (other than untoward tumourousness) causes the pituitary gland to reach its largest natural size... and why?
Saturday, 20 October 2012
Pituitary Awareness Quiz: Day 3
I have to say, I have been delighted almost beyond reason by the responses I have received so far! Today I seemed to spend a lot of my time making pies (apple crumble and puff pastry chicken pie with peppers), and playing boardgames (I don't even remember their names), it was excellent. But it left an unfortunately small amount of time for writing today's question. Nevertheless, allow me to present:
Q.3: Which of these is an alternative name for the pituitary stalk?
a) The fungible branch
b) The expungable peduncle
c) The infundibular stem
d) The peduncular pedicle
National Pituitary Awareness Month Pituitary Awareness Quiz
Day 3, Question 3
Q.3: Which of these is an alternative name for the pituitary stalk?
a) The fungible branch
b) The expungable peduncle
c) The infundibular stem
d) The peduncular pedicle
Friday, 19 October 2012
Pituitary Awareness Quiz: Day 2
Welcome to today's question about the pituitary gland! Yesterday's question was relatively easy to Google, so I thought I'd throw in a slightly more tricky one for you (and my boyfriend did the calculations!).
Q.2: Approximately how many (normal-sized) human pituitary glands could you fit in an Olympic-sized swimming pool?
a) 4 billion
b) 20 billion
c) 50 billion
d) 100 million
e) 100 billion
Anyone who provides workings to back up their answer will receive great respect. Good luck!
National Awareness Month Pituitary Awareness Quiz
Day 2 - Question 2
Q.2: Approximately how many (normal-sized) human pituitary glands could you fit in an Olympic-sized swimming pool?
a) 4 billion
b) 20 billion
c) 50 billion
d) 100 million
e) 100 billion
Anyone who provides workings to back up their answer will receive great respect. Good luck!
Thursday, 18 October 2012
Nationary Pituitary Awareness Month Pituitary Awareness Quiz
Even the most ardent readers of my blog will probably have forgotten that October is National Pituitary Awareness Month. Oh yes, ladies and gentlemen - that happy time is here again! Try to contain your excitement, please.
Last year, I looked at some of the other National Months that are held in October; this year, I felt like doing something different. But pituitary glands are tricky things to raise awareness for, especially considering that approximately eighty percent of Britons can't even spell the word "pituitary", let alone point to its location in the body.*
And then it hit me.
Fortunately, I wasn't seriously injured.
Dear readers, it's been over a year since I started this blog. Some of you have been here from the start, some of you have joined me along the way, and some of you typed "piglets in a teacup" into Google and arewondering how the hell you ended up here.** Believe me, I'm wondering too. But I feel quite strongly that all of you should have increased, improved and frankly incredible knowledge of the pituitary gland as a result of reading this blog, and now you will finally have the chance to prove it. And so, I present: The National Pituitary Awareness Month Pituitary Awareness Quiz! It's not sanctioned by any healthcare professionals, and it's not recognised as a professional medical qualification anywhere, ever - but the winner will gain both bragging points, a delightful poem about how wise they are, and my eternal respect.
Here's how it's going to work: For the remainder of the month, I will post one (probably multiple-choice) question about the pituitary gland every day.*** To be in with a chance of winning, simply post your answer in the comments section. Correct answers gain you one point. At the end of the month, I will leave a day or so for anyone who wants to join in to answer all the questions, then I'll tot up the points and announce the winner and write a short praise poem about how awesome they are.
Here's the twist: correct answers gain one point. Answers (however wildly incorrect) which include something that amuses me - a pun, rhyming couplet, accompanying picture or just shameless flattery - will get two points. Because life's not fair, and neither is my pituitary gland.
If I get more than five comments before the end of the month, I will count this quiz as a wild success, so please join in!
Q.1: Acromegaly is a rare disease caused by a growth-hormone-secreting pituitary tumour, which can lead to gigantism and excessive growth of the body's tissues. But what language is the word "acromegaly" derived from, and what does it literally mean?
Is it:
a) from the Latin acro "extremity; member of the body" and magnus "large"
b) from the Greek arka "repository; hidden place" and megaras "growth".
c) from the Greek akros "highest; extremity" and megalos "large".
It's an easy-to-Google one to start you off. Fly, my pretties, fly!
_____________________________________
* Warning: spurious fact alert.
** This is actually a genuine search that somehow resulted in my blog
coming up. I have no idea why
***In theory.
Last year, I looked at some of the other National Months that are held in October; this year, I felt like doing something different. But pituitary glands are tricky things to raise awareness for, especially considering that approximately eighty percent of Britons can't even spell the word "pituitary", let alone point to its location in the body.*
And then it hit me.
Fortunately, I wasn't seriously injured.
Dear readers, it's been over a year since I started this blog. Some of you have been here from the start, some of you have joined me along the way, and some of you typed "piglets in a teacup" into Google and arewondering how the hell you ended up here.** Believe me, I'm wondering too. But I feel quite strongly that all of you should have increased, improved and frankly incredible knowledge of the pituitary gland as a result of reading this blog, and now you will finally have the chance to prove it. And so, I present: The National Pituitary Awareness Month Pituitary Awareness Quiz! It's not sanctioned by any healthcare professionals, and it's not recognised as a professional medical qualification anywhere, ever - but the winner will gain both bragging points, a delightful poem about how wise they are, and my eternal respect.
Here's how it's going to work: For the remainder of the month, I will post one (probably multiple-choice) question about the pituitary gland every day.*** To be in with a chance of winning, simply post your answer in the comments section. Correct answers gain you one point. At the end of the month, I will leave a day or so for anyone who wants to join in to answer all the questions, then I'll tot up the points and announce the winner and write a short praise poem about how awesome they are.
Here's the twist: correct answers gain one point. Answers (however wildly incorrect) which include something that amuses me - a pun, rhyming couplet, accompanying picture or just shameless flattery - will get two points. Because life's not fair, and neither is my pituitary gland.
If I get more than five comments before the end of the month, I will count this quiz as a wild success, so please join in!
National Pituitary Awareness Month Pituitary Awareness Quiz
Day 1 - Question 1
Q.1: Acromegaly is a rare disease caused by a growth-hormone-secreting pituitary tumour, which can lead to gigantism and excessive growth of the body's tissues. But what language is the word "acromegaly" derived from, and what does it literally mean?
Is it:
a) from the Latin acro "extremity; member of the body" and magnus "large"
b) from the Greek arka "repository; hidden place" and megaras "growth".
c) from the Greek akros "highest; extremity" and megalos "large".
It's an easy-to-Google one to start you off. Fly, my pretties, fly!
_____________________________________
* Warning: spurious fact alert.
** This is actually a genuine search that somehow resulted in my blog
coming up. I have no idea why
***In theory.
Wednesday, 17 October 2012
Back to La Cura
Regular readers who have not grown tired of my recent lack of posting
may recall that a little while ago I posted a link to a website called
Open Source Cure, created by an Italian man, Salvatore Iaconesi, who has
been diagnosed with brain cancer. BBC News has recently done a piece
about the website, which has provoked a huge response in terms of both
medical advice, messages of support and artwork. Apparently the public
reaction to the website and Mr Iaconesi's interactions with various
doctors have influenced the way in which his brain surgery is going to
be carried out, and the Italian government have even picked up on the
site's popularity, and is now looking at opening up patients' medical
records.

It's quite an incredible response to see. Many people, myself included,
turn to blogging as a way of venting the frustrations of being ill and
dealing with hospitals, as a way of updating friends and family on how
we are, and as a way of connecting with other people in similar
situations. When you have a rare illness like thyrotropinoma, it's
seriously unlikely that you'll know anyone who's been through the same
thing in real life, so it's natural to reach out to others online. But the concept of
seeking not only support and tips but also actual medical advice on
treatments and surgical techniques from complete strangers - from the
whole world - is a pretty unique approach. Given the difficulty that
people with rare medical conditions can have in accessing doctors with
sufficient (or indeed any) experience in the treatment of their illness,
perhaps it's something that will become increasingly common.
may recall that a little while ago I posted a link to a website called
Open Source Cure, created by an Italian man, Salvatore Iaconesi, who has
been diagnosed with brain cancer. BBC News has recently done a piece
about the website, which has provoked a huge response in terms of both
medical advice, messages of support and artwork. Apparently the public
reaction to the website and Mr Iaconesi's interactions with various
doctors have influenced the way in which his brain surgery is going to
be carried out, and the Italian government have even picked up on the
site's popularity, and is now looking at opening up patients' medical
records.

It's quite an incredible response to see. Many people, myself included,
turn to blogging as a way of venting the frustrations of being ill and
dealing with hospitals, as a way of updating friends and family on how
we are, and as a way of connecting with other people in similar
situations. When you have a rare illness like thyrotropinoma, it's
seriously unlikely that you'll know anyone who's been through the same
thing in real life, so it's natural to reach out to others online. But the concept of
seeking not only support and tips but also actual medical advice on
treatments and surgical techniques from complete strangers - from the
whole world - is a pretty unique approach. Given the difficulty that
people with rare medical conditions can have in accessing doctors with
sufficient (or indeed any) experience in the treatment of their illness,
perhaps it's something that will become increasingly common.
Tuesday, 16 October 2012
October's Injection
I went to the hospital on the first of October to have my latest lanreotide injection. It feels like ages ago now! They're a long-acting formulation, so they last for about four weeks in your system, meaning that the next one is due on or around the 29th October. Of course, I don't have a date or an appointment to get the next one. That would make life far too easy!
I have slightly begun to wonder whether the hospital has enrolled me in some kind of secret government trial without my knowledge and against my will, where they gradually increase their level of administrative incompetence every month, and see how long it takes before I start frothing at the mouth.
Anyway, I went for the injection and dragged my boyfriend along to the hospital with me, to keep me company during the (usually fairly lengthy) wait. Of course, this was the one time that there was virtually no hanging around, and I was whisked away into the endocrine nurses' lair almost as soon as I arrived. I did request that he get me a coffee while he waited - but as he is not a drinker of hot caffeinated beverages, he became overwhelmed by the variety of -accinos on offer, and consequently I had to buy it myself afterwards. So I decided to publicly shame him on this blog. Friends and family, be warned.
The injection itself wasn't too bad, I'm not going to repeat my usual "sweet jesus guys it's a MASSIVE FREAKING NEEDLE" post (oh wait; yes I am. It's HUGE). The nurse giving me the injection was very apologetic and really somewhat incensed by the delays that I'd had in trying to get it - apparently not only had it taken longer than usual to garner various signatures because everyone had been on holiday, but they also managed to lose the paperwork at some point. Ah, the NHS at its finest.
The long and the short of it is that I'm pretty well determined to write a letter of complaint to the hospital, finally. I don't enjoy writing letters and I've kind of been putting it off, but I really should do it. As anyone who reads this blog regularly must be aware, I spend a frankly alarming amount of time chasing the hospital up about things they've promised to arrange and then entirely failed or forgotten to deliver - and aside from anything else, even ignoring their track history, it really can't be acceptable that patients' treatment is delayed by a month because a doctor goes on holiday. If I go on holiday from my [insert mystery job here] and something needs to get signed off, my colleagues can sign it off for me after checking my notes. I appreciate that medicine is a rather more high-risk calling than [insert lowly job here] but I refuse to believe that in hospitals across the country no-one gets treatment in August because half the doctors are sunning themselves in the south of France.
Post-hospital (and post-coffee) we trudged back to my house, limping slightly (well, I was limping). Unfortunately, having to go all the way to the hospital for these injections means much more walking immediately afterwards, and my leg is quite sore for a few hours. By the evening though, I was fully recovered and even went dancing, which was excellent!
I have slightly begun to wonder whether the hospital has enrolled me in some kind of secret government trial without my knowledge and against my will, where they gradually increase their level of administrative incompetence every month, and see how long it takes before I start frothing at the mouth.
Anyway, I went for the injection and dragged my boyfriend along to the hospital with me, to keep me company during the (usually fairly lengthy) wait. Of course, this was the one time that there was virtually no hanging around, and I was whisked away into the endocrine nurses' lair almost as soon as I arrived. I did request that he get me a coffee while he waited - but as he is not a drinker of hot caffeinated beverages, he became overwhelmed by the variety of -accinos on offer, and consequently I had to buy it myself afterwards. So I decided to publicly shame him on this blog. Friends and family, be warned.
The injection itself wasn't too bad, I'm not going to repeat my usual "sweet jesus guys it's a MASSIVE FREAKING NEEDLE" post (oh wait; yes I am. It's HUGE). The nurse giving me the injection was very apologetic and really somewhat incensed by the delays that I'd had in trying to get it - apparently not only had it taken longer than usual to garner various signatures because everyone had been on holiday, but they also managed to lose the paperwork at some point. Ah, the NHS at its finest.
The long and the short of it is that I'm pretty well determined to write a letter of complaint to the hospital, finally. I don't enjoy writing letters and I've kind of been putting it off, but I really should do it. As anyone who reads this blog regularly must be aware, I spend a frankly alarming amount of time chasing the hospital up about things they've promised to arrange and then entirely failed or forgotten to deliver - and aside from anything else, even ignoring their track history, it really can't be acceptable that patients' treatment is delayed by a month because a doctor goes on holiday. If I go on holiday from my [insert mystery job here] and something needs to get signed off, my colleagues can sign it off for me after checking my notes. I appreciate that medicine is a rather more high-risk calling than [insert lowly job here] but I refuse to believe that in hospitals across the country no-one gets treatment in August because half the doctors are sunning themselves in the south of France.
Post-hospital (and post-coffee) we trudged back to my house, limping slightly (well, I was limping). Unfortunately, having to go all the way to the hospital for these injections means much more walking immediately afterwards, and my leg is quite sore for a few hours. By the evening though, I was fully recovered and even went dancing, which was excellent!
Thursday, 11 October 2012
Return of the Living Head
And I'm back! Apologies for another long delay. I have not forsaken you, dear reader. As you may remember, I started a new job in September and am somewhat busier than in my previous job - consequently, while I used to spend my lunchtimes peacefully penning delightful (and lengthy) blogposts, I now spend them staring blankly at stories about singing mice on BBC News and resting my poor beleaguered brain. I also moved house around the same time, and so instead of spending my evenings huddled at my desk typing furiously, I now spend them watching Heroes (curse you, housemates!).*
At my workplace this morning, however, I spent twenty minutes looking for a room that didn't exist. I didn't find it, but the experience has left me feeling the need to express myself. And that, dear reader, is where you come in.
However, as it's been so long I thought maybe instead of boring you all with a massive post catching up on everything that's happened, I would provide a quick summary on my progress with my various medical issues. So here goes:
Getting lanreotide injection: 100% complete
Getting funding for future injections: Data insufficient
Getting surgery date: 0% complete
Getting appointment with surgeon: 0% complete
Getting appointment with ENT re. sinusitis: 0% complete
Getting pissed off with all the delays: 100% complete
Writing a letter to the hospital to complain about it: 0% complete
Being cured: 0% complete
As you can see, great progress has not been made, although I have at least had a lanreotide injection now. It was a month late because things kept managing to go wrong at the hospital's end, which is frustrating enough, but worse is the fact that no-one ever bothered to update me on what was happening, which meant that I had to keep calling to try to find out what was going on.
Anyway, more on that another time, this is meant to be my super-quick return of the jedi from the deadi post. Adieu!
____________________________________________________
* I should point out that I don't just watch Heroes at home. Since moving in, I have also gone stiltwalking, learned how to spin a plate on a stick, covered my own leg in henna tattoos and made the world's worst lemon drizzle cake. But Heroes has featured quite heavily.
At my workplace this morning, however, I spent twenty minutes looking for a room that didn't exist. I didn't find it, but the experience has left me feeling the need to express myself. And that, dear reader, is where you come in.
However, as it's been so long I thought maybe instead of boring you all with a massive post catching up on everything that's happened, I would provide a quick summary on my progress with my various medical issues. So here goes:
Getting lanreotide injection: 100% complete
Getting funding for future injections: Data insufficient
Getting surgery date: 0% complete
Getting appointment with surgeon: 0% complete
Getting appointment with ENT re. sinusitis: 0% complete
Getting pissed off with all the delays: 100% complete
Writing a letter to the hospital to complain about it: 0% complete
Being cured: 0% complete
As you can see, great progress has not been made, although I have at least had a lanreotide injection now. It was a month late because things kept managing to go wrong at the hospital's end, which is frustrating enough, but worse is the fact that no-one ever bothered to update me on what was happening, which meant that I had to keep calling to try to find out what was going on.
Anyway, more on that another time, this is meant to be my super-quick return of the jedi from the deadi post. Adieu!
____________________________________________________
* I should point out that I don't just watch Heroes at home. Since moving in, I have also gone stiltwalking, learned how to spin a plate on a stick, covered my own leg in henna tattoos and made the world's worst lemon drizzle cake. But Heroes has featured quite heavily.
Tuesday, 25 September 2012
IMFW: Headache? Painkiller!
If television advertising has taught me one thing over the past few years, it's that headaches are evil red pulsating blobs inside your head, and that if you have one, you can cure it with NUROFEN and that NUROFEN will heal all your achy ills and NUROFEN PLUS is there for when you have an exceptional amount of pain that needs to be killed, because humans are WEAK and liable to developing red pulsating headblobs at any moment.
I think that advert was for Nurofen, anyway...
If actual real life has taught me anything, it's that you should go to the doctor if you have headaches regularly, and also that being allergic to paracetamol is annoying if you're then put on medication which means you can't take aspirin or ibuprofen.
If the BBC has taught me anything this week, it's that painkillers can actually cause headaches, which I had no idea about. We all know you should be careful not to OD on paracetamol (but did you know that paracetamol is actually the commonest drug overdose in the UK, and accounts for a massive 48% of all poisoning admissions to hospital?), yet in fact even at non-toxic doses painkillers can cause what are known as medication overuse headaches. NICE has recently issued new guidance to health professionals in England and Wales on the subject.
If headaches get worse after a couple of months of regular use of painkillers, it's possible that they have developed into medication overuse headaches, and unfortunately the only cure is to go cold turkey and see if they improve - but at first they'll get worse. Also known as rebound headaches, they can be a serious problem, often occurring in people who already suffer from migraine or other chronic headache conditions, and who may have no idea that they're taking painkillers too frequently.
{kind=link}
I think that advert was for Nurofen, anyway...
If actual real life has taught me anything, it's that you should go to the doctor if you have headaches regularly, and also that being allergic to paracetamol is annoying if you're then put on medication which means you can't take aspirin or ibuprofen.
If the BBC has taught me anything this week, it's that painkillers can actually cause headaches, which I had no idea about. We all know you should be careful not to OD on paracetamol (but did you know that paracetamol is actually the commonest drug overdose in the UK, and accounts for a massive 48% of all poisoning admissions to hospital?), yet in fact even at non-toxic doses painkillers can cause what are known as medication overuse headaches. NICE has recently issued new guidance to health professionals in England and Wales on the subject.
If headaches get worse after a couple of months of regular use of painkillers, it's possible that they have developed into medication overuse headaches, and unfortunately the only cure is to go cold turkey and see if they improve - but at first they'll get worse. Also known as rebound headaches, they can be a serious problem, often occurring in people who already suffer from migraine or other chronic headache conditions, and who may have no idea that they're taking painkillers too frequently.
Thursday, 20 September 2012
The (Im)Patient Patient
I've always had a problem with the phrase "caught like a rat in a trap". I feel it could be improved upon. Rats are smart. Rats, once caught, sometimes make it out of traps.
But they never make it out of cats.
I currently feel much like a rat in a cat. It has now been six weeks since I had an injection of lanreotide. They only last for a month. During that month I did feel much better. At one point I ran upstairs and my heartrate barely increased, even though I hadn't taken my medication that day. For me, that is a medial coup indeed.
Alas, those halcyon days are gone. I'm back to taking two or three propranolol tablets a day to keep my heartrate as normal as possible. My moments of hypoglycaemia (brought on by the lanreotide injections) have been replaced by finding the six flights of stairs to my desk much more challenging in the morning.*
As you can imagine, I am chafing under this new and irritating regime, rendered all the more irritating by the fact that if my stupid former GP's surgery didn't have such nonsensical rules then I would have had my second injection by now and all would be hunky dory. Consequently, I'm calling the hospital every week to find out what's going on. I contact one of the nurses in the endocrine department, who is lovely, and then we have a mutual guilt festival, whereby she feels guilty for not being able to give me good news and I feel guilty for making her feel guilty considering that it's not her fault in the slightest.
I called last Wednesday, at the five-weeks-since-last-injection mark, and the nurse said that she could confirm all the paperwork had finally been submitted, and she seemed optimistic that it would get approved quickly and I'd get the injection soon. I called again today but the atmosphere of optimism had sadly been replaced with uncertainty over exactly how long this would take. Apparently, if your life is not immediately threatened by the lack of medication, then it doesn’t matter that you're symptomatic and the tumour in your head could well be growing happily like an evil, greedy mushroom.** You just have to be patient.
If ever I had wondered how the word "patient" had come to have two such different meanings - meaning in the first instance, a calm endurance of difficulty, and in the second, a person receiving medical treatment - I stopped wondering some time ago, because it seems that extreme feats of patience are required pretty much as soon as you become a patient.
_________________________________________________
*I should point out that my desk is in an office which is accessed by climbing six flights of stairs and then walking along a corridor. I don't just have a desk sitting atop a massive staircase, although that would be quite awesome.
** I don't like mushrooms.
But they never make it out of cats.
I currently feel much like a rat in a cat. It has now been six weeks since I had an injection of lanreotide. They only last for a month. During that month I did feel much better. At one point I ran upstairs and my heartrate barely increased, even though I hadn't taken my medication that day. For me, that is a medial coup indeed.
Alas, those halcyon days are gone. I'm back to taking two or three propranolol tablets a day to keep my heartrate as normal as possible. My moments of hypoglycaemia (brought on by the lanreotide injections) have been replaced by finding the six flights of stairs to my desk much more challenging in the morning.*
As you can imagine, I am chafing under this new and irritating regime, rendered all the more irritating by the fact that if my stupid former GP's surgery didn't have such nonsensical rules then I would have had my second injection by now and all would be hunky dory. Consequently, I'm calling the hospital every week to find out what's going on. I contact one of the nurses in the endocrine department, who is lovely, and then we have a mutual guilt festival, whereby she feels guilty for not being able to give me good news and I feel guilty for making her feel guilty considering that it's not her fault in the slightest.
I called last Wednesday, at the five-weeks-since-last-injection mark, and the nurse said that she could confirm all the paperwork had finally been submitted, and she seemed optimistic that it would get approved quickly and I'd get the injection soon. I called again today but the atmosphere of optimism had sadly been replaced with uncertainty over exactly how long this would take. Apparently, if your life is not immediately threatened by the lack of medication, then it doesn’t matter that you're symptomatic and the tumour in your head could well be growing happily like an evil, greedy mushroom.** You just have to be patient.
If ever I had wondered how the word "patient" had come to have two such different meanings - meaning in the first instance, a calm endurance of difficulty, and in the second, a person receiving medical treatment - I stopped wondering some time ago, because it seems that extreme feats of patience are required pretty much as soon as you become a patient.
_________________________________________________
*I should point out that my desk is in an office which is accessed by climbing six flights of stairs and then walking along a corridor. I don't just have a desk sitting atop a massive staircase, although that would be quite awesome.
** I don't like mushrooms.
Tuesday, 18 September 2012
IMFW: Scintillating Scotoma
Up until recently, I had never heard of scintillating scotoma, but my boyfriend is an occasional sufferer - and although that is not so fun for him, it's certainly a handy suggestion for an Interesting Medical Fact of the Week!
The word scintillating comes from the Latin scintillare - to sparkle, glitter, gleam or flash. The word scotoma comes from the Greek for darkness. So at first etymological glance, it would appear that a scintillating scotoma is something of an oxymoron.
Medically speaking, a scintillating scotoma is a symptom which often precedes the onset of migraine, although it can also appear as an isolated symptom without headache. Wikipedia describes it as follows:
Scintillating scotoma usually begins as a spot of flickering light near or in the center of the visual fields, which prevents vision within the scotoma. The scotoma area flickers, but is not dark. The scotoma then expands into one or more shimmering arcs of white or colored flashing lights. An arc of light may gradually enlarge, become more obvious, and may take the form of a definite zigzag pattern, sometimes called a fortification spectrum, because of its resemblance to the fortifications of a castle or fort seen from above.
The visual anomaly results from abnormal functioning of portions of the occipital cortex, at the back of the brain, not in the eyes. Symptoms typically appear gradually over 5 to 20 minutes and generally last fewer than 60 minutes, leading to the headache in classic migraine with aura, or resolving without consequence in acephalgic migraine.
Sounds kind of pretty, right? Unfortunately, even if you don't get a headache or other symptoms, it does massively mess with your vision until it resolves. If you search online, you can see a selection of artist's impressions of what scintillating scotoma can look like to sufferers:

The word scintillating comes from the Latin scintillare - to sparkle, glitter, gleam or flash. The word scotoma comes from the Greek for darkness. So at first etymological glance, it would appear that a scintillating scotoma is something of an oxymoron.
Medically speaking, a scintillating scotoma is a symptom which often precedes the onset of migraine, although it can also appear as an isolated symptom without headache. Wikipedia describes it as follows:
Scintillating scotoma usually begins as a spot of flickering light near or in the center of the visual fields, which prevents vision within the scotoma. The scotoma area flickers, but is not dark. The scotoma then expands into one or more shimmering arcs of white or colored flashing lights. An arc of light may gradually enlarge, become more obvious, and may take the form of a definite zigzag pattern, sometimes called a fortification spectrum, because of its resemblance to the fortifications of a castle or fort seen from above.
The visual anomaly results from abnormal functioning of portions of the occipital cortex, at the back of the brain, not in the eyes. Symptoms typically appear gradually over 5 to 20 minutes and generally last fewer than 60 minutes, leading to the headache in classic migraine with aura, or resolving without consequence in acephalgic migraine.
Sounds kind of pretty, right? Unfortunately, even if you don't get a headache or other symptoms, it does massively mess with your vision until it resolves. If you search online, you can see a selection of artist's impressions of what scintillating scotoma can look like to sufferers:

Friday, 14 September 2012
One Year Later
It's been precisely one year since I started this blog! Here is a link to my first ever post. Ah, fond memories.
It's actually a bit of a fluke for me to be posting this, I knew I started writing about a year ago and have been meaning to check the precise date for weeks and haven't got around to it... until today. Which happens to be the one-year anniversary of the day I started boring the internet to tears with an excess of information about my pituitary tumour. And other people's pituitary tumours. And the history of pituitary tumours.
Not entirely sure how this anniversary should be celebrated, although obviously getting wasted is always a classic option. One year ago I was still getting over surgery; now I'm waiting for another surgery.* In September 2010, this blog got a grand total of 157 views; so far this month I've had just under 1,000 and we're not even halfway.
Ok, that's getting dull fast. I'll just say happy blogoversary, thanks for reading, and please force your friends to do the same. Or, if you've just started reading and you don't like what you see, your enemies.
Ciao!
__________________________________________________
*And, indeed, for the NHS to get its fat ass in gear and give me the medication I need.
It's actually a bit of a fluke for me to be posting this, I knew I started writing about a year ago and have been meaning to check the precise date for weeks and haven't got around to it... until today. Which happens to be the one-year anniversary of the day I started boring the internet to tears with an excess of information about my pituitary tumour. And other people's pituitary tumours. And the history of pituitary tumours.
Not entirely sure how this anniversary should be celebrated, although obviously getting wasted is always a classic option. One year ago I was still getting over surgery; now I'm waiting for another surgery.* In September 2010, this blog got a grand total of 157 views; so far this month I've had just under 1,000 and we're not even halfway.
Ok, that's getting dull fast. I'll just say happy blogoversary, thanks for reading, and please force your friends to do the same. Or, if you've just started reading and you don't like what you see, your enemies.
Ciao!
 |
| Have a picture of a monopod from the 1473 Nuremberg Chronicle. Because why not? |
*And, indeed, for the NHS to get its fat ass in gear and give me the medication I need.
An Open-Source Cure?
Kudos to my lovely boyfriend for this very interesting link to a website created by an Italian man with brain cancer, who requested copies of his medical files from his hospital in order to send to other hospitals and doctors for their opinions, only to find that they were in proprietary formats which he could not open on his computer. Being computer savvy, he managed to convert them into open formats so that he can share his information with everyone, online. And he's posted them on his website.
It might sound weird, this idea of posting medical records online, when these are documents that we're used to treating with the utmost confidentiality, but already he has had responses from doctors - and the idea is that everyone is encouraged to use the data to create a cure, whether that's a doctor suggesting treatment, an artist creating artworks, videos, poems... you name it. Other people with similar conditions can send in their own data, if they wish, to be added to the site.
The author of the website had some very interesting thoughts about how the way in which his data is treated parallels the way in which his disease has been treated:
"The data formats which I was "forced" to hack is in a peculiar state of harmony with the common definition of "disease/illness".
The definition of "diseases" is "reserved" to doctors. Often using words which we don't understand and, most important of all, touching only a part of the human condition, which is made from body, but also of spirit and sociality.
The DICOM format is open, yes, but in a very "peculiar" condition of openness: it is like the openness of the words which they use to tell you about your health condition, and with which they descrive and actuate their version of the "cure": you can't understand it, you can't reuse it, you can't combine it with other possibilities. It is thought for "experts" and "professionals" (of one single type), leaving little space for other possibilites for expression and socialization."
It's interesting to consider the possibility that the sacred doctrine of doctor-patient confidentiality may, in some cases, end up mitigating against patients having the ability to take charge of their own healthcare, or seek the widest possible range of medical opinions on their condition. Now that so many hospital systems and even procedures are digitised, there's clearly a balance to be struck between protecting patients' private information, and making it so inacessible that patients are unable to view their own data.
Historically, medical education and knowledge has been very much the preserve of the privileged few, and patients weren't necessarily expected to understand their own conditions. With the rise of the internet, it's so much easier for patients to be informed about their own illness - some might say too easy - and thus it seems terribly ironic that the same medium enabling greater patient choice and freedom should simultaneously be creating new and unwelcome restrictions on their ability to use their own data in whatever way they desire.
Posting your medical records on the internet for all to see may not be everyone's cup of tea. But it should still be an option if that's what you want to do.
Check it out: http://artisopensource.net/cure/
It might sound weird, this idea of posting medical records online, when these are documents that we're used to treating with the utmost confidentiality, but already he has had responses from doctors - and the idea is that everyone is encouraged to use the data to create a cure, whether that's a doctor suggesting treatment, an artist creating artworks, videos, poems... you name it. Other people with similar conditions can send in their own data, if they wish, to be added to the site.
The author of the website had some very interesting thoughts about how the way in which his data is treated parallels the way in which his disease has been treated:
"The data formats which I was "forced" to hack is in a peculiar state of harmony with the common definition of "disease/illness".
The definition of "diseases" is "reserved" to doctors. Often using words which we don't understand and, most important of all, touching only a part of the human condition, which is made from body, but also of spirit and sociality.
The DICOM format is open, yes, but in a very "peculiar" condition of openness: it is like the openness of the words which they use to tell you about your health condition, and with which they descrive and actuate their version of the "cure": you can't understand it, you can't reuse it, you can't combine it with other possibilities. It is thought for "experts" and "professionals" (of one single type), leaving little space for other possibilites for expression and socialization."
It's interesting to consider the possibility that the sacred doctrine of doctor-patient confidentiality may, in some cases, end up mitigating against patients having the ability to take charge of their own healthcare, or seek the widest possible range of medical opinions on their condition. Now that so many hospital systems and even procedures are digitised, there's clearly a balance to be struck between protecting patients' private information, and making it so inacessible that patients are unable to view their own data.
Historically, medical education and knowledge has been very much the preserve of the privileged few, and patients weren't necessarily expected to understand their own conditions. With the rise of the internet, it's so much easier for patients to be informed about their own illness - some might say too easy - and thus it seems terribly ironic that the same medium enabling greater patient choice and freedom should simultaneously be creating new and unwelcome restrictions on their ability to use their own data in whatever way they desire.
Posting your medical records on the internet for all to see may not be everyone's cup of tea. But it should still be an option if that's what you want to do.
Check it out: http://artisopensource.net/cure/
Saturday, 8 September 2012
Denied
My god! Apparently I haven't published a post since the 31st of August and it's now the 8th September! I am well behind schedule. In fairness, in the past week I have been to a wedding, started a new job and moved house so I feel like I have some kind of excuse for my laxness. On the other hand, excuse schmoose! Shame on me.
I do in fact have an update on my health situation, although not a particularly jolly one. Regular readers will remember that the NHS is proving remarkably loath to pay for the treatment that fixes me. I need regular injections, one every month, which normalise my hormone levels and make me feel much more chirpy, and also possibly stop the tumour growing which would be A Good Thing. They also cost about £750 a pop.
I got the first injection just over a month ago. The hospital then had a month to wrangle who was going to pay for the next one. I was booked in to go back on Wednesday morning for the next injection. Surprise, surprise, on Tuesday afternoon I got a phone call from one of the nurses informing me that they had not sorted out the funding issue and it would be "one or two weeks" before I could have the next one. Past experience would suggest that "one or two weeks" could be anything up to several months.
It's very frustrating, because the injections make such a difference to my symptoms. I massively cut down on the amount of medication I was taking for my heart, to the point where some days I didn't need it at all. I was sleeping better, my nails were better, my eyelashes got thicker (weirdly when my thyroid hormone levels are too high they tend to thin out!), everything was improving. And now I just have to wait, slowly feeling worse and worse all the time.
It's hard not to feel annoyed at my new GP for starting this whole mess by refusing to prescribe it despite letters from the hospital asking her to. I know that she was just playing by the book. But if the tumour in my head goes untreated and keeps growing and makes me more ill it's just more hassle for the NHS in the long run. I really don't care who pays for it. But can SOMEONE please get it sorted?
I do in fact have an update on my health situation, although not a particularly jolly one. Regular readers will remember that the NHS is proving remarkably loath to pay for the treatment that fixes me. I need regular injections, one every month, which normalise my hormone levels and make me feel much more chirpy, and also possibly stop the tumour growing which would be A Good Thing. They also cost about £750 a pop.
I got the first injection just over a month ago. The hospital then had a month to wrangle who was going to pay for the next one. I was booked in to go back on Wednesday morning for the next injection. Surprise, surprise, on Tuesday afternoon I got a phone call from one of the nurses informing me that they had not sorted out the funding issue and it would be "one or two weeks" before I could have the next one. Past experience would suggest that "one or two weeks" could be anything up to several months.
It's very frustrating, because the injections make such a difference to my symptoms. I massively cut down on the amount of medication I was taking for my heart, to the point where some days I didn't need it at all. I was sleeping better, my nails were better, my eyelashes got thicker (weirdly when my thyroid hormone levels are too high they tend to thin out!), everything was improving. And now I just have to wait, slowly feeling worse and worse all the time.
It's hard not to feel annoyed at my new GP for starting this whole mess by refusing to prescribe it despite letters from the hospital asking her to. I know that she was just playing by the book. But if the tumour in my head goes untreated and keeps growing and makes me more ill it's just more hassle for the NHS in the long run. I really don't care who pays for it. But can SOMEONE please get it sorted?
Friday, 31 August 2012
Acromegaly Community
I am a little overexcited that the piece I wrote recently about Kate Woodward, the girl with acromegaly who sued the NHS, has been posted on the Acromegaly Community blog. It's an excellent website that I have frequently read in the past so I was delighted to hear from them when they asked to post the article! (Thanks, guys). It's definitely highly recommended if you have acromegaly. If you live in the US, it also has some very useful information on financial support for your prescriptions, information on discrimination in the workplace, and medical studies which are currently recruiting.
Plus, if you're passing by you can click 'like' on my post >.>
Plus, if you're passing by you can click 'like' on my post >.>
Wednesday, 29 August 2012
The Sound of Striped Hooves
Around a year or so ago, an interesting thing happened to me. I was in the car with my mother, we were driving down the motorway, and there was a car pulling a horsebox in front of us. We were going rather faster than the horsebox, and as we passed it, I looked inside and saw… a zebra. It was only a glimpse and it confused the hell out of me for a moment, but I am still sure it was a zebra, not a horse, inside that horsebox.* At first I was slightly worried I might be going mad, but my mother pointed out that there are plenty of zoos and animal parks around the place and presumably they must transport their zebras somehow.
Folk of a medical persuasion will probably see where I am going with this, but I promise it is an entirely true story, the proof of which is that it took months and months for it to occur to me that I could use it on this blog. What can I say? I am slow.
Healthy people are probably wondering why I am blathering about hoofed african mammals instead of my usual cheery chat about tumours, but fret not. All shall be revealed.
A zebra is, as Wikipedia (and, I believe, Scrubs) so nobly tells us, the medical term for a surprising diagnosis, which rather begs the question of what we should call those stripey ponies running around in nature documentaries. It comes from the aphorism that when you hear hoofbeats behind you, you don't expect to see a zebra. This is a wise observation which is totally inapplicable to anyone who lives in the African plains, but as it was coined by an American doctor in the 1940s, this oversight may perhaps be forgiven. The point is that when a doctor is presented with a set of symptoms which may be caused by a common illness or an uncommon one, the logical assumption should be that the patient most likely has the more common illness - even though there may be a temptation to go with the more dramatic diagnosis.
I have noticed this idea of being a medical zebra popping up in a few blogs by other people with rare pituitary tumours, particularly in those with Cushing's disease - possibly this is related to the fact that one of the symptoms of Cushing's is the development of dramatic stretchmarks of a stripey and thus zebra-like nature. A few further examples - here, here and here.
I guess I count as a medical zebra myself; my symptoms of hyperthyroidism such as tachycardia, hair loss and frenzied blogging** would normally be considered as indicating Graves disease or something - and even when the more common thyroid malfunctions were ruled out, it was considered more likely that I had a condition called Resistance to Thyroid Hormone than thyrotropinoma. But no, my body had picked the most unusual way it could think of to break down, and I was neither a horse, nor a pony, deer, mule, donkey, nor any one of a number of hoofed creatures which are more common in the UK than zebras.
Medical zebras are a tricky subject, on the whole, and there's obviously a balance to be struck. While it can be frustrating for those of us with unusual conditions to think that we waited a long time for a diagnosis, it would be far worse if doctors went around ignoring common diagnoses in favour of the weird ones. Equally though, doctors should be aware that just because something's weird and unusual doesn't mean it's not sitting in front of you - as anyone who's come face-to-face with Boris Johnson could tell you.
It's enough to make you wonder how rare your condition would have to be before you were considered a medical okapi...
______________________________________________
*Unless someone had painted a horse to look like a zebra. Which would be a pretty weird thing to do.
**Hint: one of these is not actually a symptom.
Folk of a medical persuasion will probably see where I am going with this, but I promise it is an entirely true story, the proof of which is that it took months and months for it to occur to me that I could use it on this blog. What can I say? I am slow.
Healthy people are probably wondering why I am blathering about hoofed african mammals instead of my usual cheery chat about tumours, but fret not. All shall be revealed.
A zebra is, as Wikipedia (and, I believe, Scrubs) so nobly tells us, the medical term for a surprising diagnosis, which rather begs the question of what we should call those stripey ponies running around in nature documentaries. It comes from the aphorism that when you hear hoofbeats behind you, you don't expect to see a zebra. This is a wise observation which is totally inapplicable to anyone who lives in the African plains, but as it was coined by an American doctor in the 1940s, this oversight may perhaps be forgiven. The point is that when a doctor is presented with a set of symptoms which may be caused by a common illness or an uncommon one, the logical assumption should be that the patient most likely has the more common illness - even though there may be a temptation to go with the more dramatic diagnosis.
I have noticed this idea of being a medical zebra popping up in a few blogs by other people with rare pituitary tumours, particularly in those with Cushing's disease - possibly this is related to the fact that one of the symptoms of Cushing's is the development of dramatic stretchmarks of a stripey and thus zebra-like nature. A few further examples - here, here and here.
 |
| A group of Cushing's sufferers at a recent conference. |
 |
| Neighbours of Lord Rothschild may not only have expected to see zebras when they heard the sound of hoofbeats, but also had to leap out of their way. |
It's enough to make you wonder how rare your condition would have to be before you were considered a medical okapi...
{kind=link}
______________________________________________
*Unless someone had painted a horse to look like a zebra. Which would be a pretty weird thing to do.
**Hint: one of these is not actually a symptom.
Monday, 27 August 2012
IMFW: Thyrotoxic Period Paralysis
Today's Interesting Medical Fact of the Week is about thyrotoxic periodic paralysis, a curious malady occurring mainly in men of Japanese, Vietnamese, Chinese, Korean Thai and Filipino descent - and Native Americans are also at greater risk, as they share a genetic background with East Asian people. The condition causes attacks of muscle weakness and paralysis and usually occurs in the presence of high thyroid hormone levels (hyperthyroidism) and low potassium levels (hypokalemia).
The attacks of paralysis can be brought on by exercise, drinking alcohol and eating food high in carbohydrates or salt, and they can be dangerous if they lead to respiratory failure or irregular heartbeat. This condition can be treated by first correcting the hypokalemia, then the hyperthyroidism; once treatment has achieved normal thyroid levels, this usually leads to a complete resolution of the problem.
Thyrotoxic period paralysis is commonly associated with Graves Disease, although other illnesses which lead to high thyroid levels (including TSH-producing pituitary adenoma... yay!) can also cause the condition. It's not fully understood and there is still confusion over why males are predominantly affected despite the fact that overactive thyroid problems are more common in women.
The attacks of paralysis can be brought on by exercise, drinking alcohol and eating food high in carbohydrates or salt, and they can be dangerous if they lead to respiratory failure or irregular heartbeat. This condition can be treated by first correcting the hypokalemia, then the hyperthyroidism; once treatment has achieved normal thyroid levels, this usually leads to a complete resolution of the problem.
Thyrotoxic period paralysis is commonly associated with Graves Disease, although other illnesses which lead to high thyroid levels (including TSH-producing pituitary adenoma... yay!) can also cause the condition. It's not fully understood and there is still confusion over why males are predominantly affected despite the fact that overactive thyroid problems are more common in women.
Friday, 24 August 2012
Lyrically Sick
Apologies for the lack of blogging of late, I have been on holiday! I cunningly set my Interesting Medical Fact of the Week to automatically post on Monday, having written it last week, but don't be fooled. I spent the weekend at the Edinburgh Festival, which was amazing, and this week I'm at my boyfriend's house many miles away, so although technically I have had access to a computer, my impetus to blog has not really been there and also, nothing that exciting and medical has happened.
But no more! I have decided to get cracking on a post I intended to write some time ago, in which I will look at the lyrics of popular songs and attempt to diagnose the singer on the basis of the symptoms they describe experiencing when viewing their beloved.
Before you judge me, perhaps I should clarify that the song selection should in no way be held as representative of my own musical preferences and was chosen purely on the basis of medically interpretable lyrics.
First up we have:
So come on, spin me around
I don’t wanna go home
Cause when you hold me like this
You know my heart skips, skips a beat
Olly Murs describes experiencing ectopic beats, or the sensation of a skipped or missed heartbeat - not to be confused with ectopic beets, which is when a beetroot grows in your fallopian tube. This is a very common form of cardiac arryhthmia, and indeed is really nothing to be concerned about in a healthy adult.
However, Mr Murs indicates that his palpitations occur only when the object of his affection spins him around and holds him in a particular way. This could indicate that he is suffering from postural orthostatic tachycardia syndrome, a condition in which the body struggles to deal with the changes in blood pressure occasioned by a change from a lying-down to an upright posture, or even by more minor changes in posture, and the heartrate increases dramatically as a result. Olly Murs may find his symptoms improved by increasing his fluid intake, taking regular exercise and wearing strong support tights.
Can't read my,
Can't read my,
No he can't read my poker face.
Ms Gaga reports that the apple of her eye is unable to read her poker face. Sad to say, he may well be suffering from a condition called prosopagnosia, also known as 'face blindness', in which the ability to recognise faces is affected. Sufferers may be unable to recognise even their own face, and are forced to rely on other qualities such as voice, gait, and clothing to tell people apart from one another. Ms Gaga would be able to help her friend to recognise her by, for example, picking a distinctive piece of clothing and always wearing it around him. Perhaps a hat made out of a telephone would suffice.
Boy, you're an alien
Your touch so foreign
It's supernatural
Extraterrestrial
In this song, Katy Perry appears to be under the impression that her significant other is from another planet. In this, it would seem likely that she is suffering from Capgras syndrome, in which the sufferer has the delusion that a close friend or relative has been replaced by an identical imposter. It may occur in cases of schizophrenia, dementia and brain injury, and it has been suggested that the Capgras delusion is in a sense the opposite of prosopagnosia, in that the person's ability to consciously recognise someone's face is intact, but they are lacking the unconscious emotional response to seeing the person's face.
Alas, that is all for now as I am totally out of inspiration. I may continue at some later date. Suggestions for songs/medical conditions greatly appreciated!
But no more! I have decided to get cracking on a post I intended to write some time ago, in which I will look at the lyrics of popular songs and attempt to diagnose the singer on the basis of the symptoms they describe experiencing when viewing their beloved.
Before you judge me, perhaps I should clarify that the song selection should in no way be held as representative of my own musical preferences and was chosen purely on the basis of medically interpretable lyrics.
First up we have:
So come on, spin me around
I don’t wanna go home
Cause when you hold me like this
You know my heart skips, skips a beat
Olly Murs describes experiencing ectopic beats, or the sensation of a skipped or missed heartbeat - not to be confused with ectopic beets, which is when a beetroot grows in your fallopian tube. This is a very common form of cardiac arryhthmia, and indeed is really nothing to be concerned about in a healthy adult.
However, Mr Murs indicates that his palpitations occur only when the object of his affection spins him around and holds him in a particular way. This could indicate that he is suffering from postural orthostatic tachycardia syndrome, a condition in which the body struggles to deal with the changes in blood pressure occasioned by a change from a lying-down to an upright posture, or even by more minor changes in posture, and the heartrate increases dramatically as a result. Olly Murs may find his symptoms improved by increasing his fluid intake, taking regular exercise and wearing strong support tights.
Can't read my,
Can't read my,
No he can't read my poker face.
Ms Gaga reports that the apple of her eye is unable to read her poker face. Sad to say, he may well be suffering from a condition called prosopagnosia, also known as 'face blindness', in which the ability to recognise faces is affected. Sufferers may be unable to recognise even their own face, and are forced to rely on other qualities such as voice, gait, and clothing to tell people apart from one another. Ms Gaga would be able to help her friend to recognise her by, for example, picking a distinctive piece of clothing and always wearing it around him. Perhaps a hat made out of a telephone would suffice.
{kind=link}
Boy, you're an alien
Your touch so foreign
It's supernatural
Extraterrestrial
In this song, Katy Perry appears to be under the impression that her significant other is from another planet. In this, it would seem likely that she is suffering from Capgras syndrome, in which the sufferer has the delusion that a close friend or relative has been replaced by an identical imposter. It may occur in cases of schizophrenia, dementia and brain injury, and it has been suggested that the Capgras delusion is in a sense the opposite of prosopagnosia, in that the person's ability to consciously recognise someone's face is intact, but they are lacking the unconscious emotional response to seeing the person's face.
Alas, that is all for now as I am totally out of inspiration. I may continue at some later date. Suggestions for songs/medical conditions greatly appreciated!
Monday, 20 August 2012
IMFW: Harvey Cushing
This week's IMFW is really more like an IMPW - an Interesting Medical Person of the Week. Harvey Williams Cushing is often regarded as the "father of modern neurosurgery".
An American descended from a long line of doctors, he was born in Ohio in 1869. After studying medicine, he went on to study surgery at the famous Johns Hopkins Hospital just after it had opened, then spent time in Europe before returning to Johns Hopkins as an associate professor in surgery. As well as writing about medicine, he was a talented medical illustrator and several of his drawings were published in textbooks - and as if that wasn't enough, he received the Pulitzer Prize for Biography for his biography of his mentor, William Osler.
Cushing's first monograph was on the subject of the pituitary, and on this blog, you'll have heard Cushing's name from one of his most famous discoveries, the disease named after him - Cushing's Disease; a tumour of the pituitary gland which secretes ACTH (adrenocorticotrophic hormone) and causes a range of symptoms including weight gain, bruising, sweating, high blood pressure and diabetes. Being a modest chap, he had originally named it "polyglandular syndrome", but his name stuck. However, this was far from his only contribution to medicine:
- He introduced blood pressure measurement to America
- He used x-rays to diagnose brain tumours
- He developed medical instruments which are still in use today, including the Cushing Forcep which is used during cranial surgery, the Cushing clip - a small clip for blood vessels to stop bleeding during surgery, which dramatically decreased mortality rates - and the use of electrocautery which he developed with W.T. Bovie, a physicist
- Along with a colleague, Ernest Codman, Cushing devised the first anaesthetic chart to help surgeons and anaesthetists monitor pulse, temperature and breathing - an innovation which was widely adoped
- Cushing pioneered many new surgical techniques including the use of saline for irrigation during surgery
- He developed a surgical cure for trigeminal neuralgia
- His mortality rate was around 10% - which doesn't sound hugely impressive until you realise that before he came along, mortality rates from neurosurgery were 50 - 90% depending on which source you believe
- He developed the transsphenoidal approach for surgery of the pituitary gland
- He invented the macarena (just checking you're paying attention...)
- He identified and named the phenomena of hypopituitarism and hyperpituitarism
So Mr Harvey Williams Cushing deserves our gratitude and respect. He has thoroughly earned the bewildering array of unpleasant medical things named after him, which include: Cushing's Syndrome, Cushing's Disease, Cushing's symphalangism (a.k.a. proximal symphalangism), Cushing's Reflex resulting in Cushing's Triad (a nervous system response to increase intracranial pressure), Cushing ulcer a.k.a. Rokitansky-Cushing Syndrome, Bailey-Cushing Syndrome (he had to share that one), the Cushing forcep and Cushing clip.
An American descended from a long line of doctors, he was born in Ohio in 1869. After studying medicine, he went on to study surgery at the famous Johns Hopkins Hospital just after it had opened, then spent time in Europe before returning to Johns Hopkins as an associate professor in surgery. As well as writing about medicine, he was a talented medical illustrator and several of his drawings were published in textbooks - and as if that wasn't enough, he received the Pulitzer Prize for Biography for his biography of his mentor, William Osler.
Cushing's first monograph was on the subject of the pituitary, and on this blog, you'll have heard Cushing's name from one of his most famous discoveries, the disease named after him - Cushing's Disease; a tumour of the pituitary gland which secretes ACTH (adrenocorticotrophic hormone) and causes a range of symptoms including weight gain, bruising, sweating, high blood pressure and diabetes. Being a modest chap, he had originally named it "polyglandular syndrome", but his name stuck. However, this was far from his only contribution to medicine:
- He introduced blood pressure measurement to America
- He used x-rays to diagnose brain tumours
- He developed medical instruments which are still in use today, including the Cushing Forcep which is used during cranial surgery, the Cushing clip - a small clip for blood vessels to stop bleeding during surgery, which dramatically decreased mortality rates - and the use of electrocautery which he developed with W.T. Bovie, a physicist
- Along with a colleague, Ernest Codman, Cushing devised the first anaesthetic chart to help surgeons and anaesthetists monitor pulse, temperature and breathing - an innovation which was widely adoped
- Cushing pioneered many new surgical techniques including the use of saline for irrigation during surgery
- He developed a surgical cure for trigeminal neuralgia
- His mortality rate was around 10% - which doesn't sound hugely impressive until you realise that before he came along, mortality rates from neurosurgery were 50 - 90% depending on which source you believe
- He developed the transsphenoidal approach for surgery of the pituitary gland
- He invented the macarena (just checking you're paying attention...)
- He identified and named the phenomena of hypopituitarism and hyperpituitarism
 |
| Yes... yes, that is a skull. |
Wednesday, 15 August 2012
Girl with Acromegaly Sues NHS
A story broke some time ago about a young lady with acromegaly who sued the NHS, and won. I've been meaning to write about her for a while but I wanted to take the time to create an interesting and informative post contrasting her case with that of Kane Gorny. Alas, I have not had the time, so you'll just have to deal with a dull and uninformative post instead. Hurrah!
The story is this: Kate Woodward, an aspiring actress, developed acromegaly (i.e. a pituitary tumour secreting growth hormone, which lead to uncontrolled growth of her body) as a child, which went untreated between 2001 and 2005 as medics failed to spot the condition. She attained a final height of 6'5" aged 20, and sued the NHS for £2 million. She was awarded compensation of £1.3m.
Incidentally, the award for "least sensitive headline about this story" goes to Healthcare Today UK, which went with "Freak Growth Woman Sues NHS".*
Nice.
Her case for being awarded this level of compensation was that, as a result of her condition being untreated for so long:
- Her height and "ugliness" meant that she could no longer go into a career as an actress.
- She has psychological difficulties and feels like a "freak" because of her condition.
- She has significant problems with her bones, knees and teeth, and cannot buy normal-sized clothes.
- The condition affected her childhood, schooling and friendships.
And, most significantly:
- She wishes to receive all future treatment in the private sector.
Now, not long after this story was first brought to my attention (by a colleague, thank you!) I noticed that it had also popped up as a topic of discussion on the Pituitary Foundation's forum. For those of you who don't subscribe, one member created a poll entited something like "Should Kate Woodward be ashamed of herself?" The results of the poll were overwhelmingly that she should (although in fairness by "overwhelmingly", I mean "there were four votes in total").
Why the anger? Surely she has a fairly good case, right? Undoubtedly, when a doctor is presented with a girl who measured 5'9" at just eleven years old and keeps growing, you'd hope that it wouldn't take four years to just Google it and think "hmm, maybe we should rule out acromegaly". Although we can't know that faster treatment would have effected a cure, it might have controlled or reduced the symptoms. She will have to live with injections and monitoring and joint problems and feeling self-conscious for her whole life.
BUT.
The problem is that this is not, actually, an unusual case - at least, not within the magical world of pituitary tumours. If every person with acromegaly decided to sue the NHS for delayed diagnosis, it would be one hell of a bonus day for lawyers. If you threw in people with other often-missed pituitary conditions like Cushing's Disease and TSHoma, it would probably result in a sudden UK lawyer shortage as they all retired to small Caribbean islands. If you based the level of compensation awarded on the number of years the condition went undiagnosed, the small Caribbean islands would probably reinvent themselves as world financial hubs.
I exagerate. But the mean length of time from onset of symptoms to diagnosis of acromegaly is, according to this MedScape article, around 12 years. Even if that estimate is too high, the point is that pituitary tumour conditions can be hard to diagnose, and they are often missed because they're rare enough that doctors don't see them often, and often don't expect to see them either. Four years to diagnose a patient with acromegaly is, sadly, not uncommon. I first showed symptoms of my TSH-secreting pituitary tumour aged 17, and I didn't get a diagnosis until I was 22. (In case you're bad at maths, that's five years). Even after my superfast heartrate made it clear that Something Was Wrong, it took a year to work out what that something was.
So if there's a slight lack of sympathy from other acromegalomaniacs,** it could be because they're thinking "Damn, £2m! Wish I'd thought of that."
But I doubt it. And I'm not just saying that because they're bigger than me.***
Now I want to note right off the bat that where there is evidence of medical negligence or it takes a long time to get a diagnosis, you should complain. Vociferously. You should complain in the hope that procedures can be improved. Otherwise there's nothing to stop future patients from suffering through the same tortuous process to find out what's wrong with them. But there's a difference between seeing a problem, taking a complaint as far as necessary to fix that problem for future patients, and just suing to get as much as you can out of them. Through the normal complaints process, the hospital in question offered Miss Woodward compensation of £700k, no court appearance required. If she lives to the age of 90, that would be £10,000 medical expenses covered every year. Additionally, according to the Daily Mail, which I personally take with a pinch of salt and under the supervision of a doctor, the hospital trust had already spent £288,000 on Miss Woodward for "treatment, dental care, holidays and special footwear".
Even the £500k difference between what she was offered and what the court awarded is a big chunk of money. £500k that could have gone towards treating other patients. I need somatostatin analogue injections (probably much like those Miss Woodward takes), and if you've been reading this blog lately, you'll know that it is proving slightly tricky to persuade someone to fund them. £500k could pay for 666-and-a-bit doses of those injections. Which doesn't sound like that much, until you realise that each dose lasts for a month, so £500k worth of injections would last me for fifty-five years. And six months. Assuming I needed them continuously. And of course by that point I would be 79-and-a-half, so chances are I could be dead by then anyway.
And here's the thing. If the NHS messes up and, as a result, you end up incurring further costs in your daily life (eg. you're a professional tap dancer going into hospital for an appendectomy, and you wake up with a leg missing) then yep, you should get compensation and if they won't agree to pay it, sue them with my blessing and encouragement. If the clinical negligence of your child at birth leads to brain damage which will affect that child for their entire life, then sue for the money needed to support them. And if/when the NHS messes up so badly that it becomes a danger to other patients, and you follow through that complaints process and nothing changes, sue them until they sit up and pay attention and mend their ways.
But I am somewhat uncomfortable with suing the NHS for the loss of a career that did not yet exist, and for the costs of having exactly the same treatment as the NHS provides, but done privately. (I'm also intrigued by the concept, since she presumably did not have private health insurance before diagnosis and consequently insurers would be unlikely to cover her pre-existing condition?). I've had an MRI scan done by a private provider and done by the NHS and the experience was almost exactly the same - except the private hospital was a lot harder to get to on public transport.
I guess in some way I think that when the NHS messes up, part of the compensation is the NHS. The very fact that you live in a country where you don't have to worry about the cost of healthcare means that when the NHS makes a mistake, it - not you - ends up bearing any increased costs of your care as a result of its mistake. Perhaps in some countries when a patient gets a hospital-acquired infection, their bill from the hospital is increased - but in the UK, if a hospital gives you an infection, it has to foot the bill to try and fix it.
But it also means that when you sue an NHS hospital in the UK, you're not taking lobster off the table of a fat cat investor (well... not yet... comments about Mr Lansley on a postcard, please). You are taking money away from that hospital. Any sensible hospital trust will have a big old stash of contingency fund to cover the cost of lawsuits, but I still confess I'm uncomfortable with the idea of suing the NHS for anything less than an ironclad reason, because that money could be put to better use. It could be used to help treat someone just like you.
I don't think Kate Woodward is a bad person, and I don't think she should be ashamed of herself. I simply don't have sufficient details to form an opinion on this case, and she may well be entirely justified. But she sparks off an interesting debate. That's my opinion. What's yours?
______________________________________
*I noticed Jon Danzig, a journalist with acromegaly, took them to task for this in the comments section of the article, good on him!
** I don't know what the collective noun for "a group of people with acromegaly" is, but it should really be this.
***Common misconception: people with acromegaly only become very tall if the condition develops during childhood/adolescence. If it develops in adulthood, it will lead to bone and soft tissue growth but usually won't increase height much, if at all.
The story is this: Kate Woodward, an aspiring actress, developed acromegaly (i.e. a pituitary tumour secreting growth hormone, which lead to uncontrolled growth of her body) as a child, which went untreated between 2001 and 2005 as medics failed to spot the condition. She attained a final height of 6'5" aged 20, and sued the NHS for £2 million. She was awarded compensation of £1.3m.
Incidentally, the award for "least sensitive headline about this story" goes to Healthcare Today UK, which went with "Freak Growth Woman Sues NHS".*
Nice.
Her case for being awarded this level of compensation was that, as a result of her condition being untreated for so long:
- Her height and "ugliness" meant that she could no longer go into a career as an actress.
- She has psychological difficulties and feels like a "freak" because of her condition.
- She has significant problems with her bones, knees and teeth, and cannot buy normal-sized clothes.
- The condition affected her childhood, schooling and friendships.
And, most significantly:
- She wishes to receive all future treatment in the private sector.
Now, not long after this story was first brought to my attention (by a colleague, thank you!) I noticed that it had also popped up as a topic of discussion on the Pituitary Foundation's forum. For those of you who don't subscribe, one member created a poll entited something like "Should Kate Woodward be ashamed of herself?" The results of the poll were overwhelmingly that she should (although in fairness by "overwhelmingly", I mean "there were four votes in total").
Why the anger? Surely she has a fairly good case, right? Undoubtedly, when a doctor is presented with a girl who measured 5'9" at just eleven years old and keeps growing, you'd hope that it wouldn't take four years to just Google it and think "hmm, maybe we should rule out acromegaly". Although we can't know that faster treatment would have effected a cure, it might have controlled or reduced the symptoms. She will have to live with injections and monitoring and joint problems and feeling self-conscious for her whole life.
BUT.
The problem is that this is not, actually, an unusual case - at least, not within the magical world of pituitary tumours. If every person with acromegaly decided to sue the NHS for delayed diagnosis, it would be one hell of a bonus day for lawyers. If you threw in people with other often-missed pituitary conditions like Cushing's Disease and TSHoma, it would probably result in a sudden UK lawyer shortage as they all retired to small Caribbean islands. If you based the level of compensation awarded on the number of years the condition went undiagnosed, the small Caribbean islands would probably reinvent themselves as world financial hubs.
I exagerate. But the mean length of time from onset of symptoms to diagnosis of acromegaly is, according to this MedScape article, around 12 years. Even if that estimate is too high, the point is that pituitary tumour conditions can be hard to diagnose, and they are often missed because they're rare enough that doctors don't see them often, and often don't expect to see them either. Four years to diagnose a patient with acromegaly is, sadly, not uncommon. I first showed symptoms of my TSH-secreting pituitary tumour aged 17, and I didn't get a diagnosis until I was 22. (In case you're bad at maths, that's five years). Even after my superfast heartrate made it clear that Something Was Wrong, it took a year to work out what that something was.
So if there's a slight lack of sympathy from other acromegalomaniacs,** it could be because they're thinking "Damn, £2m! Wish I'd thought of that."
But I doubt it. And I'm not just saying that because they're bigger than me.***
Now I want to note right off the bat that where there is evidence of medical negligence or it takes a long time to get a diagnosis, you should complain. Vociferously. You should complain in the hope that procedures can be improved. Otherwise there's nothing to stop future patients from suffering through the same tortuous process to find out what's wrong with them. But there's a difference between seeing a problem, taking a complaint as far as necessary to fix that problem for future patients, and just suing to get as much as you can out of them. Through the normal complaints process, the hospital in question offered Miss Woodward compensation of £700k, no court appearance required. If she lives to the age of 90, that would be £10,000 medical expenses covered every year. Additionally, according to the Daily Mail, which I personally take with a pinch of salt and under the supervision of a doctor, the hospital trust had already spent £288,000 on Miss Woodward for "treatment, dental care, holidays and special footwear".
Even the £500k difference between what she was offered and what the court awarded is a big chunk of money. £500k that could have gone towards treating other patients. I need somatostatin analogue injections (probably much like those Miss Woodward takes), and if you've been reading this blog lately, you'll know that it is proving slightly tricky to persuade someone to fund them. £500k could pay for 666-and-a-bit doses of those injections. Which doesn't sound like that much, until you realise that each dose lasts for a month, so £500k worth of injections would last me for fifty-five years. And six months. Assuming I needed them continuously. And of course by that point I would be 79-and-a-half, so chances are I could be dead by then anyway.
And here's the thing. If the NHS messes up and, as a result, you end up incurring further costs in your daily life (eg. you're a professional tap dancer going into hospital for an appendectomy, and you wake up with a leg missing) then yep, you should get compensation and if they won't agree to pay it, sue them with my blessing and encouragement. If the clinical negligence of your child at birth leads to brain damage which will affect that child for their entire life, then sue for the money needed to support them. And if/when the NHS messes up so badly that it becomes a danger to other patients, and you follow through that complaints process and nothing changes, sue them until they sit up and pay attention and mend their ways.
But I am somewhat uncomfortable with suing the NHS for the loss of a career that did not yet exist, and for the costs of having exactly the same treatment as the NHS provides, but done privately. (I'm also intrigued by the concept, since she presumably did not have private health insurance before diagnosis and consequently insurers would be unlikely to cover her pre-existing condition?). I've had an MRI scan done by a private provider and done by the NHS and the experience was almost exactly the same - except the private hospital was a lot harder to get to on public transport.
I guess in some way I think that when the NHS messes up, part of the compensation is the NHS. The very fact that you live in a country where you don't have to worry about the cost of healthcare means that when the NHS makes a mistake, it - not you - ends up bearing any increased costs of your care as a result of its mistake. Perhaps in some countries when a patient gets a hospital-acquired infection, their bill from the hospital is increased - but in the UK, if a hospital gives you an infection, it has to foot the bill to try and fix it.
But it also means that when you sue an NHS hospital in the UK, you're not taking lobster off the table of a fat cat investor (well... not yet... comments about Mr Lansley on a postcard, please). You are taking money away from that hospital. Any sensible hospital trust will have a big old stash of contingency fund to cover the cost of lawsuits, but I still confess I'm uncomfortable with the idea of suing the NHS for anything less than an ironclad reason, because that money could be put to better use. It could be used to help treat someone just like you.
I don't think Kate Woodward is a bad person, and I don't think she should be ashamed of herself. I simply don't have sufficient details to form an opinion on this case, and she may well be entirely justified. But she sparks off an interesting debate. That's my opinion. What's yours?
______________________________________
*I noticed Jon Danzig, a journalist with acromegaly, took them to task for this in the comments section of the article, good on him!
** I don't know what the collective noun for "a group of people with acromegaly" is, but it should really be this.
***Common misconception: people with acromegaly only become very tall if the condition develops during childhood/adolescence. If it develops in adulthood, it will lead to bone and soft tissue growth but usually won't increase height much, if at all.
Tuesday, 14 August 2012
Hypoglycaemia time!
Had my first bout of post-lanreotide hypoglycaemia today. It's silly, you'd really think I would be used to handling it by now but it still catches me unawares now and again. Fortunately I had a delicious and nutritious dried fruit bar with me to help out, although it's not quite as good as Starburst. Mmm, Starburst.*
 In other news, since having my Somatuline Autogel injection last wednesday I have been feeling rather better; I've been able to take fewer beta blockers because my heartrate has been a little slower, which has been reeeally nice - and also slightly surprising, because my heart is usually extremely slow to react to hormone changes, as far as I can tell. Plus it has been noticeably easier to go to sleep and to get up in the mornings which oh my goodness is seriously appreciated.
In other news, since having my Somatuline Autogel injection last wednesday I have been feeling rather better; I've been able to take fewer beta blockers because my heartrate has been a little slower, which has been reeeally nice - and also slightly surprising, because my heart is usually extremely slow to react to hormone changes, as far as I can tell. Plus it has been noticeably easier to go to sleep and to get up in the mornings which oh my goodness is seriously appreciated.
Also I was reading a newspaper article about the Olympics and I got a little teary-eyed, so I guess the "overemotional" aspect of these injections has also jumped in to play. People who know me in real life, you have been warned! Don't show me pictures of sad animals or I might drown you in my tears.
____________________________________________
* No, I'm not sponsored by Starburst. I'm just hoping if I mention them enough they'll take pity on me and send me some free Starburst.
Mmm, Starburst.
Also I was reading a newspaper article about the Olympics and I got a little teary-eyed, so I guess the "overemotional" aspect of these injections has also jumped in to play. People who know me in real life, you have been warned! Don't show me pictures of sad animals or I might drown you in my tears.
____________________________________________
* No, I'm not sponsored by Starburst. I'm just hoping if I mention them enough they'll take pity on me and send me some free Starburst.
Mmm, Starburst.
Monday, 13 August 2012
IMFW: Skinny Minnie or Stressy Bessie?
My favourite medical fact of the past week has been that a study has indicated that men in stressful conditions are more likely to find larger women attractive. Presumably this should prove useful to husband-hunters everywhere - the more slender ladies can go on the prowl at yoga centres and juice bars while their heavier sisters can target office blocks and traffic jams...
In less jolly news about things that are definitely true, a man with Parkinson's was arrested at the Olympic men's cycling road race. His illness meant that he did not "visibly appear to be enjoying the event", and this coupled with his proximity to a group of protestors apparently was enough for him to be arrested for breach of the peace.
Subscribe to:
Comments (Atom)